Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Pedi� 2003/
Pediatric Clinics Amsterdam Editorial Board Outcome of severe hypernatremia caused by rotavirus gastroenteritis M. P. Gruppen1 and P. Dahlem1
lopment. Also the MRI and EEGhad completely normalized. Editorial Office Case report Published by Pediatric events Kindergeneeskunde 5th International Symposium on Leukemia and Lymphoma Department of Pediatric Intensive Care, Emma Children’s Hospital AMC,References
report of a case and review of the litera-
of infancy: an epidemiological review.
sis. Neuroimag Clin North Am1993;3:319-29
Crohn’s disease: a classic presentation? E.S. van Aalst-Cohen1 and J.A.J.M. Taminiau2 Introduction
times a day, lasting several minutes.
and not to eating nor to defecation. Case report
been seen by his general practitioner.
teritis; celiac disease; pancreatitis;inflammatory bowel disease; (abdo-minal) tuberculosis; viral infection
Department of Vascular Medicine, AMC, AmsterdamEmma Childrens’ Hospital, AMC, Amsterdam
next few months showed the follo-wing results: ESR 23 mm/hour; Hb7.1 mmol/l; MCV 74.7 Fl; iron 2.6
µmol/l; ferritin 95 µg/l; transferrin1.37 g/l; TIBC 27.5 µmol/l; leuko-cytes 11.6 x 109/l; thrombocytes 630x 109/l; LDH 146 U/l; CRP 34mg/l; albumin 27 g/l; total protein59 g/l. Liver, kidney and thyroidfunction tests were normal, urinaly-sis showed no abnormalities and thePPD was negative. Serological testswere negative for EBV, HBV, andCMV. The triple feces test was posi-tive for parasites (Entamoebe coli,Blastocystis hominis and Dienta-moebe fragilis). The stools did notcontain Helicobacter pylori antigen,contained little fat and were negativefor occult blood. The patient’s skele-tal age was 9 years and 6 months,determined with an X-ray of handand wrist. No abnormalities were
Figure 1. Endoscopy: an aphthous lesion in the stomach antrum as seen on endoscopic
with metronidazol. The patient wasalso prescribed ferrous fumaratetablets to replenish his iron stores. Continued outpatient observation(2.5 months) of the patient showedno improvement of his symptoms,and a subtle increase in gastroin-testinal symptoms. Endoscopy wasperformed because of an increasingsuspicion that the child was sufferingfrom an inflammatory bowel disease(continued failure to thrive, fever,abdominal pain, iron deficiency, lowblood protein). Upon admission toour hospital for the endoscopy, thepatient was pale and cachectic inappearance. He complained of painin his knees without redness or swel-ling. The abdominal pain was moreapparent than at the initial presenta-tion in the outpatient department,however palpation of the abdomen
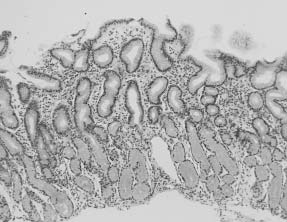
Figure 2. Pathology: a lymphoplasmacellular infiltrate in the lamina propria of thestomach antrum and two Langerhans-type giant cells.
sure was found on physical examina-tion. Laboratory results showed an
disease as seen in Crohn’s disease. Pediatric Clinics Amsterdam References
disease, but are helpful for diagnosis.
taking samples every 10 cm in thegastrointestinal tract. A febrile child with rash and arthritis: ask for recent rat exposure P.F. van Rheenen1 Case report A 15-month-old, previously healthy boy was admitted with a painful swollen right ankle joint, high fever and skin rash. The child, who had just started walking, was unable to bear weight since the day of admis- sion. Simultaneously, a rash had erupted over his palms and soles, gradually extending in proximal direction. Ten days prior to admis- sion, the patient had been bitten by a pet rat of friends of the family. A wet bandage had been applied to the injured right index finger.
ill toddler with a body temperatureof 40.4°C. His face was slightly
Figure 1. Maculopapular rash on hand palm.
puffy. A maculopapular, morbilli-form rash was seen on hand palmsand foot soles (Figure 1). The rightindex finger showed an already
healed wound. The right ankle jointwas warm and swollen. Movements
were restricted and caused severepain. Regional lymphadenopathywas not present. Blood analysis re-
vealed leukocytosis (WBC 20.5x109/l)with a shift to the left in the diffe-rential count (band neutrophils 8%).
ESR was elevated (49 mm/hr). Jointaspiration, arthrotomy and flushing
Figure 2. Characteristic course of appearance of symptoms in rat-bite fever.
were performed under general anaes-thesia. A Gram stain of the turbid
infected with S. moniliformis.
of joint aspirate isolated Streptobacil-lus moniliformis. These findings led
essential in establishing the diagnosis.
can be caused by either Streptobacil-lus moniliformis or Spirillum minor,
Europe and America, while S. minor
Complications of S. moniliformis in-
fection include endocarditis9, myo-carditis, interstitial pneumonia,
Department of Pediatrics, Emma Kinderziekenhuis AMC, AmsterdamPediatric Clinics Amsterdam
4. Konstantopoulos K, Skarpas P, Hitjazis
in children: case report and review.
tubes, impedes the growth of tient should be advised to report any
endocarditis: case report and review.
tis and numerous infectious diseases.
ments for S. moniliformis are provided. References
1. Cunningham BB, Paller AS, Katz BZ.
tial emerging disease. Int.J.Infect.Dis.
Miller L. Rat-bite fever: a case of septic
A case of Periodic fever, Aphthous stomatitis, Pharyngitis, and Adenopathy syndrome F.H. Kruisinga1 and T.W.Kuijpers1 Case report Department of Pediatrics, Emma Kinderziekenhuis AMC, Amsterdam
lesions is the hyper IgD syndrome.4In this syndrome mutations in the
tiation twice weekly for 6 weeks, lesions, arthritis and oral ulcers mayand also during an attack. ANA,
References
Behçet’s disease is rare in children.
fever, serositis, uveitis, oral and geni-
4. Editorial. Syndrome of periodic fever,
school has been reduced significantly.
adenitis (PFAPA) – What it isn’t. What
aphthous stomatitis and pharyngitis. Pediatric Clinics Amsterdam What’s new in pediatrics: Mannose Binding Lectin K.M. Dolman1 and T.W. Kuijpers1 Introduction Mannose Binding Lectin (MBL) is a plasma protein, part of the human complement system, and plays an important role in innate immunity. MBL binds to sugar residues on dif- ferent micro-organisms. This bin- ding leads to complement activation, chemotaxis of neutrophils, phagocy- tosis and finally killing of the micro- organism. The concentration of MBL in plasma is influenced by three point mutations in exon 1 of the MBL gene as well as promotor polymorphism. These mutations lead to a defective structure of the MBL molecule without biological activity. MBL deficiency predisposes to in- creased risk of infections and is asso- ciated with autoimmune diseases. Figure 1. Activation routes of the different complement pathways.Structure and function In the human immune system pro-
it takes several days before a sufficient
fore it is essential that different lectin
convertase of the classical pathway.
of MBL to a micro-organism leads organisms like viruses (i.e. influenza,
dida albicans, Staphylococcus aureus,
Aspergillus fumigatus and to a lesser
extend to Streptococcus pneumoniae
and Staphylococcus epidermidis. Some
Neisseria meningitides) are relatively
larger form to be biologically active.
ever, the MBL plasma concentrationvaries between individuals and can
Department of Pediatric Immunology, Emma Children's Hospital AMC andDepartment of Experimental Immunohematology, Sanquin Research at CLB,
MBL deficiency has also been asso-ciated with autoimmune diseases likesystemic lupus erythematosus (SLE)and rheumatoid arthritis (RA). It hasbeen postulated that MBL plays arole in the pathophysiology of SLEby defective clearance of apoptoticcells. Absence of MBL results in pro-longed presence of apoptotic cells inthe circulation and subsequent pre-sentation of nuclear material to theimmune system that results in auto-antibody formation. MBL deficiencycan also lead to decreased C3-con-vertase (C4b2a) activity and subse-quent defective clearance of circula-ting immune complexes. Low MBLplasma concentration in RA correla-tes with presentation of clinical signsat a younger age, increased erythro-
Figure 2. Tetrameric MBL (CRD: carbohydrate recognition domain; MASP:
flammatory tissue destruction anddefective mobility of the joints.
nia, gastro-enteritis, meningitis, osteo-
Conclusion
vulnerable to infections with Pseudo-monas aeruginosa or Burkholderiacepacia, and have a shorter life expec-
Clinical relevance
ciency becomes clinically important.
bably due to intrauterine infections. Pediatric Clinics Amsterdam References
10. Garred, P., Pressler, T., Lang, S., Mad-
lung disease and survival in cystic fibro-
tic fibrosis lung disease. Pediatr Pulmo-
CELEBRADO SEMINARIO SOBRE “AGROECONOMIA FAMILIAR EN EL DESARROLLO RURAL”, CON MOTIVO DEL 75 ANIVERSARIO DE LAS FACULTADES DE AGRONOMIA Y VETERINARIA DE LA UNIVERSIDAD CENTRAL DE VENEZUELA Y EL 70 ANIVERSARIO DEL INSTITUTO INTERAMERICANO DE COOPERACION PARA LA AGRICULTURA –IICA- La Facultad de Agronomía de la Universidad Central de Venezuela –Campus Maracay- fue el escenario para l
Lake Atitlan to Guatemala City Day 9 – Lake Atitlan – Guatemala CityI was up at 05:45 hoping for a spectacular sunrise. I was out on the balcony in my nightshirt and got some mildly pink shots. Try that in Canada at this time of year. I noticed that there were no screens on any of the windows and that the restaurant and bar were wide open to the outside. Perhaps bugs cannot fly at 5,000 f
 next few months showed the follo-wing results: ESR 23 mm/hour; Hb7.1 mmol/l; MCV 74.7 Fl; iron 2.6
µmol/l; ferritin 95 µg/l; transferrin1.37 g/l; TIBC 27.5 µmol/l; leuko-cytes 11.6 x 109/l; thrombocytes 630x 109/l; LDH 146 U/l; CRP 34mg/l; albumin 27 g/l; total protein59 g/l. Liver, kidney and thyroidfunction tests were normal, urinaly-sis showed no abnormalities and thePPD was negative. Serological testswere negative for EBV, HBV, andCMV. The triple feces test was posi-tive for parasites (Entamoebe coli,Blastocystis hominis and Dienta-moebe fragilis). The stools did notcontain Helicobacter pylori antigen,contained little fat and were negativefor occult blood. The patient’s skele-tal age was 9 years and 6 months,determined with an X-ray of handand wrist. No abnormalities were
Figure 1. Endoscopy: an aphthous lesion in the stomach antrum as seen on endoscopic
with metronidazol. The patient wasalso prescribed ferrous fumaratetablets to replenish his iron stores.
next few months showed the follo-wing results: ESR 23 mm/hour; Hb7.1 mmol/l; MCV 74.7 Fl; iron 2.6
µmol/l; ferritin 95 µg/l; transferrin1.37 g/l; TIBC 27.5 µmol/l; leuko-cytes 11.6 x 109/l; thrombocytes 630x 109/l; LDH 146 U/l; CRP 34mg/l; albumin 27 g/l; total protein59 g/l. Liver, kidney and thyroidfunction tests were normal, urinaly-sis showed no abnormalities and thePPD was negative. Serological testswere negative for EBV, HBV, andCMV. The triple feces test was posi-tive for parasites (Entamoebe coli,Blastocystis hominis and Dienta-moebe fragilis). The stools did notcontain Helicobacter pylori antigen,contained little fat and were negativefor occult blood. The patient’s skele-tal age was 9 years and 6 months,determined with an X-ray of handand wrist. No abnormalities were
Figure 1. Endoscopy: an aphthous lesion in the stomach antrum as seen on endoscopic
with metronidazol. The patient wasalso prescribed ferrous fumaratetablets to replenish his iron stores.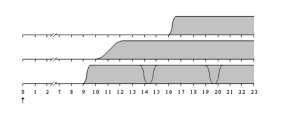
 A febrile child with rash and arthritis:
A febrile child with rash and arthritis: 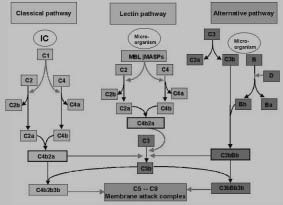 Pediatric Clinics Amsterdam
Pediatric Clinics Amsterdam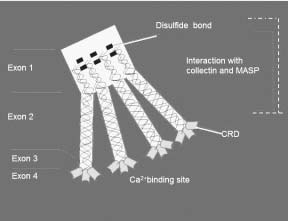 MBL deficiency has also been asso-ciated with autoimmune diseases likesystemic lupus erythematosus (SLE)and rheumatoid arthritis (RA). It hasbeen postulated that MBL plays arole in the pathophysiology of SLEby defective clearance of apoptoticcells. Absence of MBL results in pro-longed presence of apoptotic cells inthe circulation and subsequent pre-sentation of nuclear material to theimmune system that results in auto-antibody formation. MBL deficiencycan also lead to decreased C3-con-vertase (C4b2a) activity and subse-quent defective clearance of circula-ting immune complexes. Low MBLplasma concentration in RA correla-tes with presentation of clinical signsat a younger age, increased erythro-
Figure 2. Tetrameric MBL (CRD: carbohydrate recognition domain; MASP:
flammatory tissue destruction anddefective mobility of the joints.
MBL deficiency has also been asso-ciated with autoimmune diseases likesystemic lupus erythematosus (SLE)and rheumatoid arthritis (RA). It hasbeen postulated that MBL plays arole in the pathophysiology of SLEby defective clearance of apoptoticcells. Absence of MBL results in pro-longed presence of apoptotic cells inthe circulation and subsequent pre-sentation of nuclear material to theimmune system that results in auto-antibody formation. MBL deficiencycan also lead to decreased C3-con-vertase (C4b2a) activity and subse-quent defective clearance of circula-ting immune complexes. Low MBLplasma concentration in RA correla-tes with presentation of clinical signsat a younger age, increased erythro-
Figure 2. Tetrameric MBL (CRD: carbohydrate recognition domain; MASP:
flammatory tissue destruction anddefective mobility of the joints.