Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Microsoft word - anticoagulation with coumadin guidelines 2008
NEON WARFARIN ANTICOAGULATION CLINICAL GUIDELINES: 7/08 Overview
Warfarin is taken by mouth to inhibit vitamin K. This vitamin is essential for effective production ofclotting factors II, VII, IX, X, and anticoagulant proteins C&S. Warfarin is given once daily. It is monitoredby the prothrombin time and the international normalized ratio (INR). Warfarin is a narrow therapeuticindex drug (NTI). When the INR falls below 2.0 thrombosis risk increases and when the INR rises above4.0 serious bleeding risk increases. General Therapeutic recommendations for warfarin INR Range Duration of Action
Warfarin takes 4-7 days to have its optimum effect. Large loading doses do not markedly shorten thetime to achieve a full therapeutic effect but cause rapid falls in the level of protein C, which mayprecipitate paradoxical thrombosis in the first few days of warfarin therapy. The following generalrecommendations for warfarin use are made:
Initiate therapy with the estimated daily maintenance dose (2-5 mg.). Elderly or debilitated patients often require low daily doses of warfarin (2-4 mg.). Patients are confused by alternating daily doses (e.g. 7.5 and 5.0 mg). Significant changes in INR can usually be achieved by small changes in dose (15% or less). 4-5 days are required after any dose change or any new diet or drug interaction to reach the new
Frequency of Dosing Monitoring
Warfarin is monitored by the one stage prothrombin time. Prothrombin times are reported in
seconds, as a ratio of the prothrombin time in seconds to the mean normal prothrombin time ofthe laboratory, and as the international normalized ratio (INR). The INR is the most reliable way tomonitor the prothrombin time. Goals of Anticoagulation
The goal of anticoagulant therapy is to administer the lowest possible dose of anticoagulant to preventclot formation or expansion. The required degree of anticoagulation continues to evolve as studiesprovide more information about the efficacy and safety of lower doses. Current therapeutic goals forvarious disease states are summarized in Table 1.4-9 By using the lowest possible required dose ofwarfarin, the physician can minimize the risk of bleeding while providing the benefits of anticoagulation. To achieve this goal, the physician must have a working knowledge of the pharmacologic,pharmacokinetic and pharmacodynamic properties of warfarin. NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Pharmacology
Warfarin is an antagonist of vitamin K, a necessary element in the synthesis of clotting factors II, VII, IXand X, as well as the naturally occurring endogenous anticoagulant proteins C and S. These factors andproteins are biologically inactive without the carboxylation of certain glutamic acid residues. Thiscarboxylation process requires a reduced vitamin K as a cofactor. Antagonism of vitamin K or adeficiency of this vitamin reduces the rate at which these factors and proteins are produced, therebycreating a state of anticoagulation.
Therapeutic doses of warfarin reduce the production of functional vitamin Kdependent clotting factors byapproximately 30 to 50 percent. A concomitant reduction in the carboxylation of secreted clotting factorsyields a 10 to 40 percent decrease in the biologic activity of the clotting factors. As a result, thecoagulation system becomes functionally deficient.10
Pharmacokinetics
A knowledge of the pharmacokinetics of warfarin is helpful in understanding the initial response totherapy. Warfarin can be detected in the plasma one hour after oral administration, and peakconcentrations occur in two to eight hours.10 Warfarin is a racemic mixture of stereo isomers, which are99 percent bound to albumin.11 The drug is metabolized in the liver and kidneys, with the subsequentproduction of inactive metabolites that are excreted in the urine and stool.10
The half-life of racemic warfarin ranges from 20 to 60 hours. The mean plasma half-life is approximately40 hours, and the duration of effect is two to five days.10 Thus, the maximum effect of a dose occurs up to48 hours after administration, and the effect lingers for the next five days. Pharmacodynamics and Dosing Considerations Anticoagulant Activity. The anticoagulant activity of warfarin depends on the clearance of functionalclotting factors from the systemic circulation after administration of the dose. The clearance of theseclotting factors is determined by their half-lives. The earliest changes in the International NormalizedRatio (INR) are typically noted 24 to 36 hours after a dose of warfarin is administered. These changesare due to the clearance of functional factor VII, which is the vitamin Kdependent clotting factor with theshortest half-life (six hours). However, the early changes in the INR are deceptive because they do notactually affect the body's physiologic ability to halt clot expansion or form new thromboses.4
Antithrombotic Effect. The antithrombotic effect of warfarin, or the inability to expand or form clots, is notpresent until approximately the fifth day of therapy. This effect depends on the clearance of functionalfactor II (prothrombin), which has a half-life of approximately 50 hours in patients with normal hepaticfunction.
The difference between the antithrombotic and anticoagulant effects of warfarin need to be understoodand applied in clinical practice. Because antithrombotic effect depends on the clearance of prothrombin(which may take up to five days), loading doses of warfarin are of limited value.4,12 Because warfarin has along half-life, increases in the INR may not be noted for 24 to 36 hours after administration of the firstdose, and maximum anticoagulant effect may not be achieved for 72 to 96 hours.4
Loading doses of warfarin (i.e., 10 mg or more per day) may increase the patient's risk of bleedingepisodes early in therapy by eliminating or severely reducing the production of functional factor VII. Theadministration of loading doses is a possible source of prolonged hospitalization secondary to dramaticrises in INR that necessitate increased monitoring. Administration of loading doses has also beenhypothesized to potentiate a hypercoagulable state because of severe depletion of protein C. Thepractice of using loading doses should be abandoned because it has no effect on the inhibition ofthrombosis.4[corrected]
NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008
A potential paradoxic consequence of loading doses is the development of a hypercoagulable statebecause of a precipitous reduction in the concentration of protein C (approximate half-life of eight hours)during the first 36 hours of warfarin therapy.12 Thus, loading doses theoretically may cause clot formationand/or expansion by limiting the production of proteins C and S, which have shorter half-lives thanprothrombin. Consequently, the concurrent use of heparin is extremely important.
The initial dose of warfarin should approximate the chronic maintenance dose that is anticipated. In mostpatients, the average maintenance dose is 4 to 6 mg per day. Dose has an inverse relation with age. Inpatients 50 years old, the average daily dose is 6.3 mg; in patients 70 years old, the average daily doseis 3.6 mg.13
Drug interactions (discussed in detail in another section) need to be considered when warfarin therapy isinitiated. Other factors include the patient's nutritional status and gender. Patients who are malnourishedshould receive lower doses of warfarin because they probably have low vitamin K intake and decreasedserum albumin concentrations. Women generally require lower doses than men.
Patients at highest risk for complications should probably be given a smaller initial dose (2 to 4 mg perday). This dose is then titrated to the lower end of a given therapeutic range, depending on theindication. For example, the goal may be an INR of 2 to 2.5 in a patient with a history of bleeding, chronicatrial fibrillation and no additional risk factors for thrombosis.
Current recommendations for the initiation of warfarin therapy differ based on the urgency for achievingan anticoagulant effect. While warfarin is being initiated, patients who require rapid anticoagulationshould also be given unfractionated heparin or low-molecular-weight heparin intravenously orsubcutaneously in doses appropriate for the given indication.4
Heparin and warfarin therapies should overlap for approximately four to five days. The presence of atherapeutic INR does not confer protection from clot formation and expansion during the first few days ofwarfarin therapy because of the delay in the therapeutic inhibition of prothrombin.
Patients who rapidly achieve a therapeutic INR may metabolize warfarin slowly and thus may requirelower maintenance doses. The opposite holds for patients who tend to respond slowly to warfarin. 13
A small decrease in the INR is expected to occur with the discontinuation of unfractionated heparintherapy.14 (A drop of 0.3 to 0.8 in the INR has been noted by the authors of this article.)
Patients who require non-urgent anticoagulation, such as those with stable chronic atrial fibrillation, canbe started on warfarin as outpatients, without the concomitant administration of heparin.4
NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008
Recommended Therapeutic Goals for Oral Anticoagulation
Indication Duration
Prophylaxis of venous thrombosis for high-risk surgery
Thrombosis associated with antiphospholipid antibody
Acute myocardial infarction (to prevent systemic
Valvular heart disease (after thrombotic event or if the
3 weeks before and 4 weeks after atrialfibrillation if normal sinus rhythm ismaintained
*--One study6 suggested that 4 weeks may be an adequate duration of oral anticoagulant therapy in patients withoutcontinuing risk factors.
†--If oral anticoagulant therapy is elected to prevent recurrent myocardial infarction, an INR of 2.5 to 3.5 isrecommended.
‡--Depending on the type of mechanical valve (i.e., caged ball or caged disk) and the valve position (mitral), somepatients may benefit from INRs in the upper end of the range.
Information derived from references 4 through 9.
Risk Factors for Hemorrhagic Complications of Anticoagulation Therapy
• Age greater than 65 years23• Age greater than 75 years with concomitant atrial fibrillation (intracranial hemorrhage)24,25• History of gastrointestinal bleeding20• Comorbid disease states26
--Hypertension20,27--Cerebrovascular disease20--Serious heart disease4,20--Renal insufficiency20
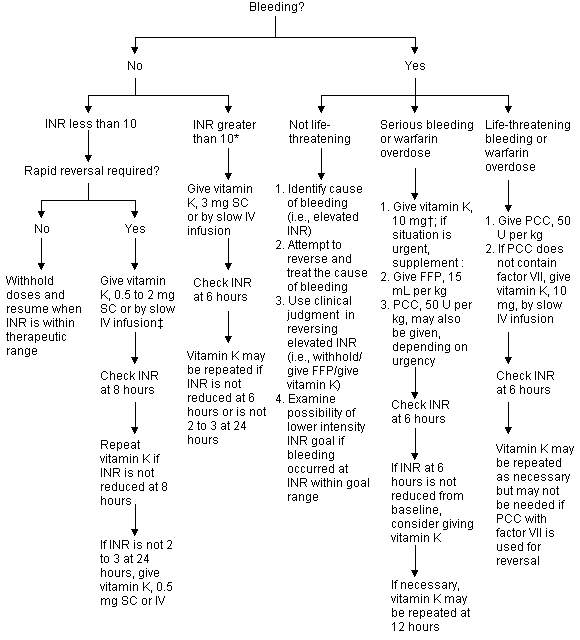
NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Warfarin-Treated Patient with Elevated INR NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Characteristics of interaction Severity Evidence Mechanism Management of interaction
acetaminophen dosage to lessthan 2 g per day; if higherdosages are used, increasedmonitoring may be necessary.
• May inducehypothyroidism orhyperthyroidism
increased sensitivity tooral anticoagulants
on a chronic barbiturateregimen is of less significance.
cholestyramine (Questran) inpatients who need a bilesequestrant.
carbamazepine is added ordiscontinued. • Increase warfarin doses whencarbamazepine is added, andreduce doses whencarbamazepine is discontinued(stabilization occurs after 4 to 6weeks). NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Severity Evidence Mechanism Management of interaction
(Cefotan) andcefmetazole (Zefazone)inhibits production ofvitamin Kdependentclotting factors
concomitant use of warfarinand cimetidine is necessary.
thromboembolism• Monitor INR frequently whenoral contraceptives are usedconcurrently with warfarin.
hypercoagulability• May have ulcerogeniceffects
use of warfarin and disulfiram. • Monitor INR if concomitantuse is necessary.
1 to 2 weeks after fluvoxamineis started. NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Severity Evidence Mechanism Management of interaction
warfarin may prolong partialthrombin time. • Be aware of small risk ofbleeding events.
warfarin and metronidazole. • Monitor INR if concomitantuse is necessary.
• Monitor INR if concomitantuse is necessary.
intermittently. • Instruct patients to takeNSAIDs with food or antacids. • Consider having patients takemisoprostol (Cytotec) to reducerisk of gastric erosions.
metabolism. • Penicillin may reducegastrointestinal florasynthesis of vitamin K.
protein-binding sites• Enhances metabolismof clotting factors
propafenone is added ordiscontinued. NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008 Severity Evidence Mechanism Management of interaction
patients to use a small dosage (325mg or less per day). • Consider having patients takemisoprostol to reduce the risk ofNSAID-induced ulceration.
of warfarin and sulfinpyrazone. • Monitor for bleeding whenconcomitant use is necessary.
warfarin• Inhibits platelet aggregation
sulfamethoxazole. • Monitor INR when concomitantuse is necessary.
related and more likely to occurwith vitamin E dosages greaterthan 800 U per day; monitor INR iflarger dosages are taken.
or dietary supplementscontaining vitamin K.
INR=International normalized ratio; HMG-CoA=3-hydroxy-3-methylglutaryl coenzyme A; NSAIDs=nonsteroidalanti-inflammatory drugs.
National prescription audit: physician specialty report, dispensed data. Plymouth Meeting, Pa.: IMS America, 1998.
Retail perspective and provider perspective audit. Plymouth Meeting, Pa.: IMS America, 1998.
Agency for Health Care Policy and Research. Life-saving treatments to prevent stroke underused. Press release, September 1995. Retrieved November 1998 from the World Wide Web at http://www.ahcpr.gov/ news/ press/stroke.htm.
Hirsh J, Dalen JE, Deykin D, Poller L, Bussey H. Oral anticoagulants: mechanism of action, clinical effectiveness, and optimal therapeuticrange. Chest 1995;108(4 Suppl):231S-46S.
Stein PD, Alpert JS, Copeland J, Dalen JE, Goldman S, Turpie AG. Antithrombotic therapy in patients with mechanical and biologicprosthetic heart valves. Chest 1995;108(4 Suppl):371S-9S [Published erratum in Chest 1996;109:592].
Levine HJ, Pauker SG, Eckman MH. Antithrombotic therapy in valvular heart disease. Chest 1995; 108(4 Suppl):360S -70S.
Schulman S, Granqvist S, Holmstrom M, Carlsson A, Lindmarker P, Nicol P, et al. The duration of oral anticoagulant therapy after a secondepisode of venous thromboembolism. N Engl J Med 1997; 336:393-8.
Laupacis A, Albers G, Dalen J, Dunn M, Feinberg W, Jacobson A. Antithrombotic therapy in atrial fibrillation. Chest 1995;108( 4Suppl):352S-9S.
Levine MN, Hirsh J, Gent M, Turpie AG, Weitz J, Ginsberg J, et al. Optimal duration of oral anticoagulant therapy: a randomized trialcomparing four weeks with three months of warfarin in patients with proximal deep vein thrombosis. Thromb Haemost 1995;74:606-11. NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008
10. Majerus PW, Broze GJ, Miletich JP, Tollefsen DM. Anticoagulant thrombolytic, and antiplatelet drugs. In: Hardman JG, Limbird LE, eds.
Goodman and Gilman's The pharmacological basis of therapeutics. 9th ed. New York: McGraw-Hill, 1996:1347-51.
11. Porter RS, Sawyer WT, Lowenthal DT. Warfarin. In: Evans WE, Schentag JJ, Jusko WJ, eds. Applied pharmacokinetics. 2d ed. Spokane,
Wash.: Applied Therapeutics, 1986:1057-104.
12. Harrison L, Johnston M, Massicotte MP, Crowther M, Moffatt K, Hirsh J. Comparison of 5-mg and 10-mg loading doses in initiation of
warfarin therapy. Ann Intern Med 1997;126:133-6.
13. Gurwitz JH, Avorn J, Ross-Degnan D, Choodnovskiy I, Ansell J. Aging and the anticoagulant response to warfarin therapy. Ann Intern Med
14. Thomas P, Fennerty A, Backhouse G, Bentley DP, Campbell IA, Routledge PA. Monitoring effects of oral anticoagulants during treatment
with heparin. Br Med J [Clin Res] 1984;288:191.
15. Ansell JE. Oral anticoagulant therapy--50 years later. Arch Intern Med 1993;153:586-96. 16. Carter BL. Therapy of acute thromboembolism with heparin and warfarin. Clin Pharm 1991;10: 503-18. 17. Norton JL, Gibson DL. Establishing an outpatient anticoagulation clinic in a community hospital. Am J Health Syst Pharm 1996;53:1151-7. 18. Wittkowsky AK. Generic warfarin: implications for patient care [Editorial]. Pharmacotherapy 1997;17: 640-3. 19. Richton-Hewett S, Foster E, Apstein CS. Medical and economic consequences of a blinded oral anticoagulant brand change at a municipal
hospital. Arch Intern Med 1988;148:806-8.
20. Routledge PA, Chapman DH, Davies DM, Rawlins MD. Pharmacokinetics and pharmacodynamics of warfarin at steady state. Br J Clin
21. Levine MN, Raskob G, Landefeld S, Hirsh J. Hemorrhagic complications of anticoagulant treatment. Chest 1995;108(4 Suppl):276S-90S. 22. Landefeld CS, Beyth RJ. Anticoagulant-related bleeding: clinical epidemiology, prediction, and prevention. Am J Med 1993;95:315-28. 23. Landefeld CS, Rosenblatt MW, Goldman L. Major bleeding in outpatients treated with warfarin: incidence and prediction by factors known
at the start of outpatient therapy. Am J Med 1989;87:144-52.
24. Albers GW. Atrial fibrillation and stroke: three new studies, three remaining questions. Arch Intern Med 1994;154:1443 -8. 25. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomized controlled
trials. Arch Intern Med 1994;154:1449-57 [Published erratum in Arch Intern Med 1994;10:2254].
26. Fihn SD, McDonell M, Martin D, Henikoff J, Vermes D, Kent D, et al. Risk factors for complications of chronic anticoagulation : a multicenter
study. Ann Intern Med 1993;118:511-20.
27. Launbjerg J, Egeblad H, Heaf J, Nielsen NH, Fugleholm AM, Ladefoged K. Bleeding complications to oral anticoagulant therapy:
multivariate analysis of 1010 treatment years in 551 outpatients. J Intern Med 1991;229:351-5.
28. Fihn SD, Callahan CM, Martin DC, McDonell MB, Henikoff JG, White RH. The risk for and severity of bleeding complications in elderly
patients treated with warfarin. Ann Intern Med 1996;124:970-9.
29. Stroke prevention in atrial fibrillation study: final results. Circulation 1991;84:527-39. 30. Hylek EM, Skates SJ, Sheehan MA, Singer DE. An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with
nonrheumatic atrial fibrillation. N Engl J Med 1996; 335:540-6.
31. Adjusted-dose warfarin versus low-intensity, fixed -dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke Prevention in
Atrial Fibrillation III randomised clinical trial. Lancet 1996; 348:633-8.
32. Havrda DE, Anderson JR, Talbert RL. Thrombosis. In: Pharmacotherapy self assessment program module 1 cardiovascular. Kansas City,
Mo.: American College of Clinical Pharmacy; 1998. Retrieved September 1998 from the World Wide Web at http:www.accp.com/psap3-des.html.
33. Warfarin. In: Drugdex. Englewood, Colo.: Micromedex Inc., 1998.
IMPORTANT: PLEASE READ PART III: CONSUMER INFORMATION What the medicinal ingredient is: Pr Lozide® (indapamide tablets) What the non-medicinal ingredients are: Read this carefully before you start taking glycerol, hydroxypropylmethyl cellulose, lactose Lozide® and each time you get a refill. This leaflet monohydrate, macrogol 6000, magnesium stearate, is a summ
EUSAPharma 606-0870A Rev F Proof No.: Manufactured by EUSA Pharma (USA), Inc. Langhorne, PA 19047 License 1829 ProstaScint® is a registered trademark of 2010 EUSA Pharma (USA), Inc. Printed in USA 606-0870A Rev F Revised 12/2010 ProstaScint® Kit TABLE 3 - INDIUM IN 111 TABLE 4 - COMPARISON OF INDIUM Repeat Scans (capromab pendetide) PHYSICAL DECAY CH
 NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008
NEON WARFARIN ANTICOAGULATION GUIDELINES July 2008