Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Oculoplasticabernardini.it
Ophthalmic Plastic and Reconstructive SurgeryVol. 17, No. 2, pp 123–1252001 The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc.
Destructive Eyelid Lesions in Sarcoidosis
Muhammad Moin, F.R.C.Ophth.,*† Robert C. Kersten, M.D.,*‡ Francesco Bernardini, M.D.,*§
*Department of Ophthalmology, University of Cincinnati, Ohio; †Department of Ophthalmology, Mayo Hospital, Lahore, Pakistan; ‡Cincinnati Eye Institute, Cincinnati, Ohio; and §Department of Ophthalmology, University of Genoa, ItalyPurpose: To report the clinical and histopathologic findings of a patient with sar-
coidosis causing bilateral destruction of the lower eyelids. Methods: Case report. Results: Bilateral destructive lower eyelid lesions and cicatricial entropion devel-
oped in a 43-year-old man with systemic sarcoidosis. Histopathology was consistentwith sarcoid granulomas. Disease progression was arrested with systemic prednisoneand methotrexate before eyelid reconstruction was performed. Conclusions: Sarcoidosis very rarely can cause destruction of full-thickness eye-
lid architecture. Active inflammation should be controlled before reconstruction.
Sarcoidosis is a multisystem disorder of un-
and neck. There were several 2- to 3-cm subcuta-
known cause characterized by noncaseating inflam-
neous nodules on his left upper arm and both legs.
matory granulomas. Ocular involvement occurs in
A chest radiograph demonstrated hilar adenopathy
25% to 50% of persons affected with sarcoidosis.1,2
consistent with pulmonary sarcoidosis. The remain-
Although skin may be involved in up to 22%3 of
der of the physical examination and medical history
cases, eyelid skin involvement is very rare. There
was noncontributory. Previous blood tests included
have been only ten previously reported cases,
an erythrocyte sedimentation rate of 15 mm and an
elevated serum angiotensin-converting enzyme of
To our knowledge, this is the first reported case
of full-thickness destruction and necrosis involving
The pertinent findings on ophthalmic examina-
both lower eyelids resulting from sarcoidosis.
tion were marked conjunctival hyperemia, leftgreater than right, with an apparent inflammatory
CASE REPORT
nodule (Fig. 1) arising from bulbar conjunctiva ad-
A 43-year-old black man was examined in July
jacent to the limbus in the left eye. There was bilat-
1998 with a 2.5-year history of intermittent red-
eral extensive destruction of lower eyelid architec-
ness, swelling, itching, and irritation of both eyes.
ture with indurated thickening, madarosis, and
After a 5-year history of an unknown inflammatory
obliteration of the eyelid margin (Fig. 2), and
condition, he was diagnosed with sarcoidosis in
marked forniceal foreshortening and symblepharon
May 1998 after a biopsy of throat and nasal polyps.
formation. The lateral 60% of the right lower eyelid
The patient also had erythematous maculopapular
showed full-thickness inflammation and destruction
lesions of the skin over the bridge of the nose, chin,
of normal landmarks. Slit-lamp and fundus exami-nations showed no evidence of anterior or posteriorsegment inflammation.
Biopsies of the eyelid, conjunctiva, and facial
skin nodules all revealed noncaseating granuloma-
Address correspondence to Dr. Robert C. Kersten, University
tous inflammation consistent with sarcoidosis. The
of Cincinnati Medical Center, Barrett Center–0670, Suite 3008,234 Goodman Street, Cincinnati, OH 45219, U.S.A.
histopathology of the eyelid showed unremarkable
FIG. 1. Conjunctival granuloma of left eye and eyelid destruc- FIG. 3. Postoperatively after reconstruction of right lower eyelid.
tion with notching apparent at initial examination.
epithelium with focal granulomas consisting of ep-
the lateral 60% of the right lower eyelid was appar-
ithelioid histiocytes, few multinucleated giant
ent (Fig. 4), and the left lower eyelid had extensive
cells, and a peripheral rim of lymphocytes and
symblepharon formation and cicatricial entropion
plasma cells in the subepithelial connective tissue
(Fig. 3). Acid fast bacilli and fungal stains were
Reconstruction of the left inferior fornix with a
mucous membrane graft and repositioning of the
Prednisone had been prescribed by the patient’s
entropic left lower eyelid was performed. The right
internist to control his systemic sarcoidosis coinci-
lower eyelid was reconstructed with a free tarsal
dent with his first visit to our office in July 1998.
graft from the left upper eyelid and transpositional
He was lost to our follow-up for 6 months, during
skin and muscle flap from the right upper eyelid for
which time methotrexate had been added and the
replacement of the anterior lamella (Fig. 5). This
prednisone dosage had been reduced. Reevaluation
resulted in a satisfactory outcome with resolution
at that time revealed the destructive inflammatory
of the trichiasis and restoration of eyelid architec-
process involving the eyelids to have resolved dra-
ture. At the last visit 2 months postoperatively, the
matically; the ulcerated areas had reepithelialized
patient still was taking methotrexate for his sys-
and the indurated thickening of the eyelid margin
temic sarcoidosis, and there was no recurrence of
had softened. Full-thickness loss of the eyelid over
Active conjunctival and eyelid inflammation with de-
FIG. 4. High-power view demonstrated noncaseating granulo-
mas consistent with sarcoidosis (H & E). Ophthalmic Plast Reconstr Surg, Vol. 17, No. 2, 2001DESTRUCTIVE EYELID LESIONS IN SARCOIDOSIS
affecting the face and eyelids.3 The case reportedherein is the first to develop destructive sarcoidosisaffecting the anterior and posterior lamella of theeyelid leading to full-thickness loss and cicatricialentropion.
Eyelid involvement in sarcoidosis may be treated
with systemic or intralesional corticosteroids, im-munosuppressants, or antimalarials2 during the ac-tive phase. Once the active inflammation has beencontrolled, surgical reconstruction may be success-fully performed. REFERENCES FIG. 5. Loss of tarsus, symblepharon, and cicatricial entropion
1. Siltzbach LE, James DG, Neville E, et al. Course and prog-
of the right lower eyelid apparent after resolution of active in-
nosis of sarcoidosis around the world. Am J Med 1985;57:
2. Brownstein S, Liszauer AD, Carey WD, Nicolle DA. Sar-
coidosis of the eyelid skin. Can J Ophthalmol 1990;25:256–9. DISCUSSION
3. Shiffner J, Sharma OP. Ulcerative sarcoidosis. Arch Der-
Ocular involvement has been reported to occur in
4. James DG, Anderson R, Langley D, et al. Ocular sarcoido-
25% to 50%1,4–7 of patients with sarcoidosis. This
sis. Br J Ophthalmol 1964;48:461–470.
5. James DG, Neville E, Langley DA. Ocular sarcoidosis.
wide variation is because of the patient population
Trans Opthalmol Soc UK 1976;96:133–139.
studied, definitions of ophthalmic involvement, and
6. Jabs DA, Johns CJ. Ocular findings in chronic sarcoidosis.
the nature of evaluations conducted. Sarcoidosis
Am J Ophthalmol 1986;102:297–301.
7. Crick RP, Hoyle C, Smellie H. The eye in sarcoidosis. Br J
can affect the eye as anterior or posterior uveitis,
Ophthalmol 1961;45:461–481.
secondary glaucoma, cataracts, lacrimal gland in-
8. Obenhauf CD, Shaw HE, Sydnor CF, et al. Sarcoidosis and
volvement, conjunctival involvement, band ker-
its ophthalmic manifestations. Am J Ophthalmol 1978;86:648–55.
atopathy, scleral plaque, optic nerve involvement,
9. Elgart ML. Cutaneous lesions of sarcoidosis. Primary
orbital involvement, and eyelid nodules.6 Cuta-
neous sarcoidosis has been reported in 12% to 27%
10. Henkind P. Sarcoidosis: an expanding ophthalmic horizon. J R Soc Med 1982;75:153–159.
of patients with systemic disease,1,2,4,5,8,9 but eyelid
11. Spencer WH. Ophthalmic pathology, an atlas and textbook.
involvement is very rare. Descriptions of the eyelid
3rd ed. Philadelphia: WB Saunders, 1985:2370–1.
lesions include “millet seed” nodules,2,10 papular
12. Duke-Elder S, MacFail PA. The ocular adnexa. Part I. Dis-eases of the eyelids. London: Kimpton, 1974:342–5.
eruptions,9,11–14 larger nodules,2,6,8–13,15 and rarely,
13. Bersani TA, Nichols CW. Intralesional triamcinolone for
lupus pernio plaques3,9,12 or swollen eyelids.14
cutaneous palpebral sarcoidosis. Am J Ophthalmol 1985;
The skin lesions in sarcoidosis characteristically
14. Hall JG, Cohen KL. Sarcoidosis of eyelid skin. Am J Oph-
manifest as elevated nodules or papules that only
very rarely ulcerate or become necrotic.3 Most
15. Diestelmeier MR, Sausker WF, Pierson DL, et al. Sarcoido-
prior reported cases of ulcerative cutaneous sar-
sis manifesting as eyelid swelling. Arch Dermatol 1982;118:356–7.
coidosis involved the lower extremities.16 There has
16. Verdegem TD, Sharma OP. Cutaneous ulcers in sarcoido-
been one report of ulcerative nodules and plaques
sis. Arch Dermatol 1987;123:1531–4. Ophthalmic Plast Reconstr Surg, Vol. 17, No. 2, 2001
R E S T A U R A N T B R E W H O U S E G R E AT B E G I N N I N G S C H I C K E N L E T T U C E W R A P S C H I C K E N P OT S T I C K E R S Marinated chicken breast diced and sautéed with Pan-seared dumplings loaded with chicken, green onions,mushrooms, water chestnuts, celery, green onions, garlic andChinese yellow chives, ginger and garlic. Served with topped with crispy wont
11 Screening and embryo selection: eliminatingChristy Nolan was deprived of oxygen at birth and suffered from cerebral palsy. Nolancouldn’t walk, talk or use his hands. He spent his short life (he died aged 43 in 2008)in a wheelchair. Until Nolan was 11 he couldn’t communicate with words at all. Then a new drugLioresal made it possible for him to use a ‘unicorn stick’ on a headband.
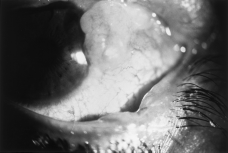

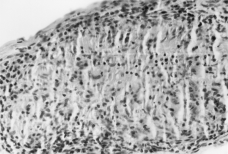
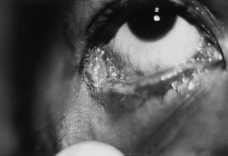 FIG. 1. Conjunctival granuloma of left eye and eyelid destruc-
FIG. 1. Conjunctival granuloma of left eye and eyelid destruc- DESTRUCTIVE EYELID LESIONS IN SARCOIDOSIS
affecting the face and eyelids.3 The case reportedherein is the first to develop destructive sarcoidosisaffecting the anterior and posterior lamella of theeyelid leading to full-thickness loss and cicatricialentropion.
DESTRUCTIVE EYELID LESIONS IN SARCOIDOSIS
affecting the face and eyelids.3 The case reportedherein is the first to develop destructive sarcoidosisaffecting the anterior and posterior lamella of theeyelid leading to full-thickness loss and cicatricialentropion.