Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Doi:10.1016/j.mimet.2007.05.002
Journal of Microbiological Methods 70 (2007) 301 – 305
A new Multi-PCR-SSCP assay for simultaneous detection of isoniazid and
rifampin resistance in Mycobacterium tuberculosis
Xiaodong Cheng a,1, Jianfang Zhang a,b,1, Liu Yang, Xiuli Xu a, Jianyun Liu a, Wenbin Yu a,
a Department of Clinical Laboratory, Xijing Hospital, the Fourth Military Medical University, Xi'an, China
b Department of Microbiology, the Fourth Military Medical University, Xi'an, China
Received 26 September 2006; received in revised form 27 April 2007; accepted 1 May 2007
Prompt detection of drug resistance in Mycobacterium tuberculosis is essential for effective control of tuberculosis (TB). We developed a
Multi-PCR-SSCP method that detects more than 80% commonly observed isoniazid (INH) and rifampin (RIF) resistance M. tuberculosis in asingle assay. The usefulness of the newly developed method was evaluated with 116 clinical isolates of M. tuberculosis. Distinct SSCP patternswere observed for different mutations and the correlation between Multi-PCR-SSCP results and DNA sequencing data was strong. Using theculture-based phenotypic drug susceptibility testing as a reference, the sensitivity of the newly developed Multi-PCR-SSCP assay was determinedto be 80% and 81.8% for INH and RIF, respectively. The specificity of the assay was 100% and 92%, for INH and RIF, respectively. Multi-PCR-SSCP provides a rapid and potentially more cost-effective method of detecting multidrug-resistant TB. 2007 Published by Elsevier B.V.
Keywords: Multidrug resistant; Tuberculosis; Multiplex PCR; Single-Strand Conformational Polymorphism Analysis (SSCP)
and transmission of resistant cases. Currently, the detection ofdrug resistance in Mycobacterium tuberculosis is primarily
Tuberculosis (TB) has a long and continuing history of
based on phenotypic drug susceptibility testing, which involves
causing worldwide morbidity and mortality. The emergence of
time consuming culture of the slow growing M. tuberculosis
multidrug-resistant TB (MDR-TB), defined as resistance to at
least isoniazid (INH) and rifampin (RIF), the 2 principal first-
line anti-TB drugs, poses an important threat to TB control.
understanding of the genetic mechanisms of M. tuberculosis
MDR-TB reduces responses to standard short-course chemo-
drug resistance, and the advancement of molecular technologies
therapy with first-line anti-TB drugs, leads to higher mortality
in recent years, have allowed the development of more rapid
and treatment failure rates, and increases the period of
molecular methods to detect mutations in genes implicated in
Most of the established methods for detecting drug resistance
of MDR-TB occurred worldwide in 2000, accounting for 3.2%
are based on single gene or single drug testing. However, it is clear
of all new TB cases (). Prompt detection of anti-
that the simultaneous detection of genetic mutations implicated
TB drug resistance is essential for controlling the development
in both INH and RIF resistance would provide a more accurate
and spread of MDR-TB, as it facilitates appropriate and timely
assessment of MDR-TB. The reverse line blot assay described by
delivery of anti-TB therapy, reducing overall cost of treatment
is the first reported attempt to combinedifferent targets in a single assay for prediction of multiple anti-TB drug resistance. Following Mokrousov's report,
⁎ Corresponding author. Tel.: +86 29 84775455; fax: +86 29 82527499.
described the use of a molecular beacon to simultaneous-
1 Both authors contributed equally to this work.
ly detect INH and RIF resistance-associated mutations in
0167-7012/$ - see front matter 2007 Published by Elsevier B.V.
X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
RIF. All of the 12B medium vials used in the test were pre-tested on a BACTEC 460TB instrument to establish a CO2atmosphere in the vial and to screen out any vials with a GI(Growth Index) of 20 or more. Bacterial suspension (0.1 mlactively growing M. tuberculosis cultures in 12B medium, GI500-799) was used to inoculate each of the BACTEC 12Bmedium vials containing the drugs. For the control vial, a 1:100dilution, made by transferring 0.1 ml of the suspension into9.9 ml of Diluting Fluid (Becton Dickinson and Company,Sparks, MD) was used. After mixing thoroughly by inverting at
Fig. 1. Multi-PCR-SSCP electrophoresis gel fragment patterns. Note: The lane
least 10 times, 0.1 ml of this dilution was used to inoculate the
MR, MI and MK represents rpoB, inhA and katG gene of H37Rv, respectively. MR has 3 ssDNA bands and the reason may be that there are different alleles. MI
control 12B medium vial (without a drug). The vials were
has 1 ssDNA band and it may because the 2 ssDNA has affinis three-
incubated at 37 ± 1 °C and tested daily at approximately the
dimensional conformation. Lane M represents multi-PCR-SSCP of H37Rv.
same time each day (± 2 h) on a BACTEC 460TB. When the
Lanes 1–7 represent multi-PCR-SSCP of clinical isolates. Lines 1 and 4 have no
control vials reached a GI of 30 or more, the results were
mutations; lines 2 and 5 have katG mutation; line 3 has rpoB and katG
interpreted as follows: If the ΔGI was less in the drug vial than
mutations; line 6 has inhA and katG mutations; line 7 has all three genesmutations.
the control, the population was deemed susceptible, if more, itwas considered resistant.
MDR-TB was defined as resistance to at least INH and RIF.
M. tuberculosis complex, from cultures and smear positive sputa.
To ensure the reliability of the phenotypic susceptibility testing
In addition, reported direct detection of
results, we performed each phenotypic drug susceptibility
multiple RIF and INH resistance mutations in M. tuberculosis
testing twice at different times, using the same test system.
respiratory samples using real-time PCR. established a multiplex allele-specific PCR (MAS-PCR) method
that simultaneously detected INH, RIF, and ethambutol (EMB)resistance-associated genetic mutations. Here we report the
M. tuberculosis genomic DNA was isolated from each
development of a Multi-PCR-SSCP (Single-Strand Conforma-
culture using a standard phenol:chloroform method. Cultured
tional Polymorphism Analysis) method that simultaneously
M. tuberculosis was transferred to a 1.5 ml Eppendorf tube,
detects INH and RIF resistance-associated genes katG, inhA,
pelleted by centrifugation (12,000×g, 5 min) and suspended in
and rpoB in a single assay, at a lower cost, and using less
0.36 ml of Marmur's solution (0.1 M NaCl, 0.01 M EDTA, pH
demanding techniques and more economical equipment than the
8.0). SDS (40 μl of 5% solution), 2 μl proteinase K (20 mg/ml),
and 2 μl RNase A (20 mg/ml) were added to the suspension. The M. tuberculosis lysate was incubated at 37 °C overnight.
An equal volume of buffer-saturated phenol was added to thedigest and thoroughly mixed by vortexing for 10 min. The top
phase was transferred to a clean tube after centrifugation(12,000×g, 5 min) and extracted with an equal volume of
For this study we used a convenience sample of 116
chloroform:isoamyl alcohol (24:1) by vortexing for 10 min, and
M. tuberculosis clinical isolates obtained from Xi'an Chest
centrifuging (12,000×g, 5 min). The top phase was transferred
Hospital. Each isolate represented a different patient. The
to a clean tube, and 0.1 volume of 3 M sodium acetate (pH 4.8)
identification of M. tuberculosis complex strains was based on
plus 2.5 volumes of absolute ethanol were added. After
conventional methods, including the niacin production test and
vortexing briefly, the mixture was chilled at −20 °C for 2 h
the nitrate reduction test, etc. As the purpose of the study was to
and centrifuged at 12,000×g for 15 min. The pellet was washed
develop a method for rapid detection of drug resistance-
with 0.5 ml of 70% ethanol, dried, and suspended in 200 μl
associated mutations of M. tuberculosis isolates, rather than to
distilled water. The presence of genomic DNA was confirmed
describe the prevalence of genetic mutations, all the available
resistant isolates and pan-sensitive isolates were included. Strain H37Rv (ATCC27294) served as the source of wild-type
PCR primers for amplifying M. tuberculosis drug resistance genes
A proportion method based on the BACTEC 460 radiometric
system (Becton Dickinson and Company, Sparks, MD) was
used for drug susceptibility testing. Aliquots of 0.1 ml drug
solution were added to 4 ml BACTEC 12B medium vials and
2307 5′-CAGACG TTG ATC AAC ATC CG-3′ 305
prepared for final concentrations of 0.1 μg/ml INH and 2 μg/ml
X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
2.4. Establishment of the multi-PCR technique
testing as the reference standard, we assessed the sensitivity andspecificity of the Multi-PCR-SSCP for detection of INH and RIF
The design of DNA oligonucleotide primers used for PCR
resistance. Sensitivity is defined as the probability of Multi-PCR-
amplification was based on the published genome sequence of
SSCP testing positive for drug resistance-associated mutations if
the resistance was found by culture. Specificity is defined as the
mutations in M. tuberculosis genes that are associated with drug
probability of Multi-PCR-SSCP testing negative if the resistance
was not found by culture. The reproducibility of the Multi-PCR-
The amount of each primer pair used in this assay was first
SSCP was examined by repeating the assay for all the study
optimized to achieve maximum amplification in separate reactions
isolates. The sequence results for M. tuberculosis H37Rv were
using the same PCR program and reaction conditions. Next, the
used as the reference for sequence comparison.
amount of each primer pair in the Multi-PCR was balanced toachieve acceptable amplification of all target genes. For each
Multi-PCR reaction, a standard 25 μl reaction mixture was used. Each reaction mix included 6 primers: 25 pmol in 1 μl, respectively.
The other reagents included in each reaction mix were 2 μl of200 μmol/l deoxyribonucleotide mix, 2.5 μl of Mg2+-free 10× PCR
Based on the phenotypic drug susceptibility testing results,
reaction buffer, 2.5 μmol/l MgCl2 1 μl, 1 μl Taq Polymerase Mix,
70 of the 116 isolates were identified as INH resistant, including
5 μl DNA solution containing 50 ng DNA template, and 7.5 μl
62 MDR-INH resistant and 8 non-MDR-INH resistant isolates.
PCR-grade water. The thermocycling parameters included an ini-
Of the 116 isolates tested, 66 were identified as RIF resistant,
tial denaturing at 95 °C for 5 min, 35 cycles of 95 °C for 30 s, 50 °C
including 62 MDR-RIF resistant and 4 non-MDR-RIF resistant.
for 30 s, and 72 °C for 45 s, and a final extension at 72 °C for 7 min.
Forty-two isolates were pansensitive.
The PCR products were examined for banding patterns by 2.0%agarose gel electrophoresis in 1× TAE buffer.
2.5. Single-Strand Conformational Polymorphism Analysis
The three genes, katG, inhA and rpoB, in the 116 clinical
isolates and H37Rv strain were amplified successfully in single
The amplified DNA was mixed with an equal volume of
formamide loading dye (97% formamide, 20 mmol/l EDTA and
0.05% bromphenol blue), denatured at 95 °C for 5 min, chilled
on ice for 1 min and loaded onto 16 cm × 18 cm, 10%
acrylamide:bisacrylamide (49:1) gels containing 0.2% glycerol.
Electrophoresis was performed using Protean II xi cells (Bio-
Rad Laboratories), at 400 V for 5 min, then 200 V 16–20 h
below 15 °C in 1× TBE buffer. The gels were silver-stained
used to provide reference wild type patterns on each gel.
2.6. Cloning of PCR amplimers and DNA sequencing
Amplimers were cloned into a PGEM T-Easy vector
(Promega, Madison, WI), and transformed into competent
Escherichia coli cells, following the protocol recommended by
the manufacturer. For each transformation, 3 clones were
selected and incubated overnight in LB broth at 37 °C in a
shaking rotary incubator (225 rpm). Plasmids from the selected
clones were extracted using a QIAprep Spin Miniprep kit
(Qiagen), and identified by EcoRI digestion, then sequenced in
both directions using M13 forward and reverse primers and an
Applied Biosystems DNA sequencer (Model 3700 or 3730).
2.7. Evaluation of the Multi-PCR-SSCP assay
Correlations between the DNA sequences and Multi-PCR-
SSCP results were determined to evaluate the usefulness of Multi-
PCR-SSCP in determining genetic mutations in clinical isolates.
Using the results of culture-based phenotypic drug susceptibility
X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
PCR reactions, except in the case of 4 katG deletion mutants.
specificities of the Multi-PCR-SSCP and DNA sequencing
Compared to strain H37Rv, 46 isolates had katG gene
methods for detecting INH and RIF resistance, and MDR, were
mutations, 14 had inhA mutations and 58 had rpoB mutations.
assessed, using culture results as a reference. The specificities
Thirty-eight isolates had simultaneous katG and rpoB mutations
and sensitivities of the Multi-PCR-SSCP determined for each
and 4 isolates had both inhA and rpoB mutations. Four isolates
testing group were similar to the corresponding specificities and
had inhA and katG mutations and 2 isolates had mutations in all
Of the 70 isolates that were INH-resistant by culture, 56 were
identified as INH-resistant by Multi-PCR-SSCP, resulting in a
detection sensitivity of 80%. Four of the 8 non-MDR INH-resistant isolates showed mutant patterns, 4 had wild type
Partial katG gene sequencing revealed mutations in 48/70
patterns. The specificity of Multi-PCR-SSCP for INH-resis-
(68.6%) INH-resistant isolates, including 44/62 (71.0%) MDR
tance detection was 100%, as 46 isolates that were susceptible
isolates and 4/8 (50%) non-MDR-INH-resistant isolates. The 4
to INH by culture all showed the expected wild-type SSCP
MDR-INH-resistant isolates had complete katG deletions,
based on the reproducible absence of PCR product. The other
For RIF resistance detection, the sensitivity of the Multi-
44 isolates possessed 46 point mutations, 4 base insertions and 4
PCR-SSCP assay was 81.8% with the identification of 54 of the
deletion mutations Ten isolates had two mutations.
66 culture-proven RIF-resistant isolates. Of the 50 culture-
Sequencing of the partial inhA gene revealed 13 point
proven RIF-susceptible isolates, 4 had the SSCP pattern of a
mutations and 1 single base deletion within 8 codons in 24
resistant strain, producing a specificity of 92% for RIF de-
isolates (), accounting for 24/70 (34.3%) of the total
tection. Mutations at codons 516 and 531 of the rpoB gene were
INH-resistant isolates. Of the 22 INH-resistant isolates with no
found in the 4 isolates by DNA sequencing. However, results of
mutation in the sequenced region of the katG gene, 12 isolates
repeated phenotypic drug susceptibility testing still classified
had mutations in the inhA gene. Of the 10 isolates with no
these 4 isolates as RIF-susceptible.
mutations in both genes, 6 were MDR isolates and 4 were non-
Of the 62 culture-proven MDR isolates, 44 were identified as
MDR INH-resistant isolates. That means 56/62 (90.3%) of the
MDR by Multi-PCR-SSCP and 46 by DNA sequencing. All of
MDR isolates and 4/8 (50%) of the non-MDR INH-resistant
the 54 non-MDR isolates defined by culture were classified as
isolates had mutations in the katG and/or inhA genes ().
non-MDR isolates by Multi-PCR-SSCP. The sensitivity of the
Sequencing of the 304-bp central region of the rpoB gene
Multi-PCR-SSCP method for MDR detection was 71.0%. Spe-
revealed point mutations at 8 different codons in 60 isolates.
Most mutations were found at codons 531, 526, and 516. Inaddition, 2 point mutations were detected at codon 528. Four
isolates were found to have dual mutations at 2 different codons,either codons 516 and 526, or 531 and 528. Two non-MDR
Our objective was to develop a molecular assay that allows
INH-resistant isolates and 2 pansensitive isolates had mutations
simultaneous detection of M. tuberculosis resistance to multiple
at codons 526 (). Of the 66 RIF-resistant isolates, 10
anti-TB drugs, INH and RIF, the 2 determining drugs for MDR-
MDR isolates had no mutations at this region of the rpoB gene.
TB. We developed a Multi-PCR-SSCP that targets the 3 genefragments in which INH, and RIF resistance-associated muta-
tions are most frequently observed. Detection sensitivity and thespecificity of the new method were assessed in comparison with
Culture-based phenotypic drug susceptibility testing is cur-
the culture-based phenotypic method, using 116 clinical isolates
rently used as the standard. Therefore the sensitivities and
of M. tuberculosis. The results of this study indicated that thisnewly developed method has potential to identify more than80% RIF or INH resistant TB isolates in 24–48 h.
The reverse line blot assay reported by Mokrousov et al.,
Sensitivity and specificity of Multi-PCR-SSCP assay and DNA sequencing fordetecting M. tuberculosis resistance to INH, RIF among 116 clinical isolates
which was the first attempt to detect multiple drugs in a singleassay, but it only included known hot-spot region mutations.
Compared to the reverse line blot assay, the MAS-PCR assay
detection of INH resistance-associated mutations in settings
where the prevalence of the commonly seen mutations is high
among the resistant clinical isolates. However, it only targeted 6
reported the use of molecular beacons for
simultaneous detection of INH and RIF resistance-associated
mutations in M. tuberculosis from cultures and smear-positive
sputa. This assay targets the same genomic loci as the MAS-
PCR. The molecular beacons assay is clearly a useful method
X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
for the rapid detection of mutations implicated in INH and RIF
resistance if resources are available. Compared with molecularbeacon-based detection, the MAS-PCR method is almost equal-
Bassam, B.J., Caetano-Anolles, G., Gresshoff, P.M., 1991. Fast and sensitive
ly efficient in terms of detecting the commonly seen genetic
silver staining of DNA in polyacrylamide gels. Anal. Biochem. 196 (1),80–83 Jul.
mutations implicated in INH and RIF resistance. However, the
Canetti, G., Fox, W., Khomenko, A., Mahler, H.T., Menon, N.K., Mitchison,
MAS-PCR can not include all mutations in the gene. Multi-
D.A., et al., 1969. Advances in techniques of testing mycobacterial drug
PCR-SSCP is not based on pre-defined or known mutations, so
sensitivity and the use of sensitivity tests in tuberculosis control programs.
it may improve the sensitivity of detection. Multi-PCR-SSCP
Bull. World Health Organ., Suppl. 41, 21–43.
combines 3 tests into a single assay, thereby substantially in-
Cole, S.T., Brosch, R., Parkhill, J., Garnier, T., Churcher, C., Harris, D., et al.,
1998. Deciphering the biology of Mycobacterium tuberculosis from the
creasing the efficiency, and significantly reducing the cost, of
complete genome sequence. Nature 396 (6707), 190 Nov 12.
detection. In addition, Multi-PCR-SSCP is less technically de-
Dye, C., Espinal, M.A., Watt, C.J., Mbiaga, C., Williams, B.G., 2002. Worldwide
manding and requires less expensive equipment, making it more
incidence of multidrug-resistant tuberculosis. J. Infect. Dis. 185, 1197–1202.
accessible for resource-limited countries.
Laszlo, A., Rahman, M., Raviglione, M., Bustreo, F., 1997. Quality assurance
A major limitation to molecular genetic detection of drug
program for drug susceptibility testing of Mycobacterium tuberculosis in theWHO/IUATLD Supranational Laboratory Network: first round of profi-
resistance by any technique is that such tests generally only detect
ciency testing. Int. J. Tuberc. Lung Dis. 1, 231–238.
known mutations. Because not all mutations conferring resistance
Libonati, J.P., Stager, C.E., Davis, J.R., Siddiqi, S.H., 1988. Direct antimicrobial
to anti-TB drugs are known, and prevalence of mutations may
drug susceptibility testing of Mycobacterium tuberculosis by the radiometric
vary by geographic area, identification of resistance-associated
method. Diagn. Microbiol. Infect. Dis. 10, 41–48.
mutations can be informative, but lack of a mutation in the target
Lin, S.Y., Probert, W., Lo, M., Desmond, E., 2004. Rapid detection of isoniazid
and rifampin resistance mutations in Mycobacterium tuberculosis complex
sequence must be interpreted with caution.
from cultures or smear-positive sputa by use of molecular beacons. J. Clin.
The Multi-PCR-SSCP cannot completely replace the culture-
based phenotypic susceptibility test because of the limitation
Marin, M., de Viedma, D.G., Ruiz-Serrano, M.J., Bouza, E., 2004. Rapid direct
mentioned above. However, it provides a rapid screening tool
detection of multiple rifampin and isoniazid resistance mutations in Myco-
for the majority of resistant isolates. Therefore, it may still be an
bacterium tuberculosis in respiratory samples by real-time PCR. Anti-microb. Agents Chemother. 48, 4293–4300.
important complementary method for TB drug susceptibility
Mokrousov, I., Bhanu, N.V., Suffys, P.N., Kadival, G.V., Yap, S.F., Cho, S.N.,
et al., 2004. Multicenter evaluation of reverse line blot assay for detection of
Another limitation of this test, particular to the current study, is
drug resistance in Mycobacterium tuberculosis clinical isolates. J. Microbiol.
that we used purified M. tuberculosis genomic DNA extracted from
cultured M. tuberculosis. Therefore, further optimization and
Schluger, N.W., 2000. The impact of drug resistance on the global tuberculosis
epidemic. Int. J. Tuberc. Lung Dis. 4, S71–S75.
evaluation of this method for direct detection of M. tuberculosis
Schneider, E., Castro, K.G., 2003. Tuberculosis trends in the United States,
drug resistance mutations in clinical specimens of TB patients
1992–2001. Tuberculosis (Edinb) 83, 21–29.
remains an important focus for future studies.
WHO, 2000. Anti-tuberculosis drug resistance in the world. Report No. 2: 7
Prevalence and Trends. The World Health Organization, Geneva, Switzerland.
Yang, Z., Durmaz, R., Yang, D., Gunal, S., Zhang, L., Foxman, B., et al., 2005.
Simultaneous detection of isoniazid, rifampin, and ethambutol resistance ofMycobacterium tuberculosis by a single multiplex allele-specific polymer-
We thank Dr. Duan Yan of Xi'an Chest Hospital for collecting
ase chain reaction (PCR) assay. Diagn. Microbiol. Infect. Dis. 53, 201–208.
bacteria strains. We thank all the staff of the clinical microbiologiclaboratory for providing assistance in the experiment.
Sjukvården, folkhemmet och folkhälsan? Helsingborg 2006-12-09 Trots att 1,5 miljoner svenskar är drabbade utbildas nästan inga allergiläkare. Det saknas i dag beräkningar av den totala samhällsekonomiska kostnaden för allergiska sjukdomar, men det finns nya siffror som visar på att enbart astma kostar det svenska samhället sex miljarder kronor om året. Trots detta saknas
FACULTE DE MEDECINE Bulletin d’information trimestriel sur l’actuali té du Centre de Recherche Clinique (CRC) neurological or psychological illness. Patients were also excluded if they had a history of depression necessitating hospitalisation, two or more recurrent episodes of depression, or suicide Mettez-vous dans la peau d’un cadre d’une firme pharmaceutique, respons

 Journal of Microbiological Methods 70 (2007) 301 – 305
A new Multi-PCR-SSCP assay for simultaneous detection of isoniazid and
rifampin resistance in Mycobacterium tuberculosis
Xiaodong Cheng a,1, Jianfang Zhang a,b,1, Liu Yang, Xiuli Xu a, Jianyun Liu a, Wenbin Yu a,
a Department of Clinical Laboratory, Xijing Hospital, the Fourth Military Medical University, Xi'an, China
b Department of Microbiology, the Fourth Military Medical University, Xi'an, China
Received 26 September 2006; received in revised form 27 April 2007; accepted 1 May 2007
Prompt detection of drug resistance in Mycobacterium tuberculosis is essential for effective control of tuberculosis (TB). We developed a
Multi-PCR-SSCP method that detects more than 80% commonly observed isoniazid (INH) and rifampin (RIF) resistance M. tuberculosis in asingle assay. The usefulness of the newly developed method was evaluated with 116 clinical isolates of M. tuberculosis. Distinct SSCP patternswere observed for different mutations and the correlation between Multi-PCR-SSCP results and DNA sequencing data was strong. Using theculture-based phenotypic drug susceptibility testing as a reference, the sensitivity of the newly developed Multi-PCR-SSCP assay was determinedto be 80% and 81.8% for INH and RIF, respectively. The specificity of the assay was 100% and 92%, for INH and RIF, respectively. Multi-PCR-SSCP provides a rapid and potentially more cost-effective method of detecting multidrug-resistant TB.
Journal of Microbiological Methods 70 (2007) 301 – 305
A new Multi-PCR-SSCP assay for simultaneous detection of isoniazid and
rifampin resistance in Mycobacterium tuberculosis
Xiaodong Cheng a,1, Jianfang Zhang a,b,1, Liu Yang, Xiuli Xu a, Jianyun Liu a, Wenbin Yu a,
a Department of Clinical Laboratory, Xijing Hospital, the Fourth Military Medical University, Xi'an, China
b Department of Microbiology, the Fourth Military Medical University, Xi'an, China
Received 26 September 2006; received in revised form 27 April 2007; accepted 1 May 2007
Prompt detection of drug resistance in Mycobacterium tuberculosis is essential for effective control of tuberculosis (TB). We developed a
Multi-PCR-SSCP method that detects more than 80% commonly observed isoniazid (INH) and rifampin (RIF) resistance M. tuberculosis in asingle assay. The usefulness of the newly developed method was evaluated with 116 clinical isolates of M. tuberculosis. Distinct SSCP patternswere observed for different mutations and the correlation between Multi-PCR-SSCP results and DNA sequencing data was strong. Using theculture-based phenotypic drug susceptibility testing as a reference, the sensitivity of the newly developed Multi-PCR-SSCP assay was determinedto be 80% and 81.8% for INH and RIF, respectively. The specificity of the assay was 100% and 92%, for INH and RIF, respectively. Multi-PCR-SSCP provides a rapid and potentially more cost-effective method of detecting multidrug-resistant TB.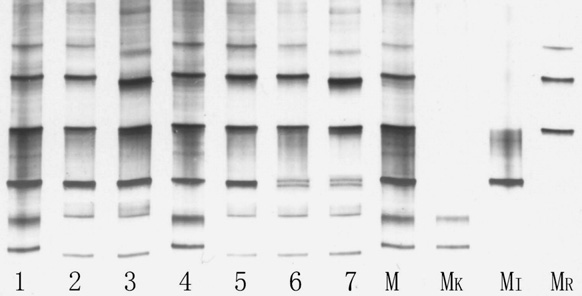 X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
RIF. All of the 12B medium vials used in the test were pre-tested on a BACTEC 460TB instrument to establish a CO2atmosphere in the vial and to screen out any vials with a GI(Growth Index) of 20 or more. Bacterial suspension (0.1 mlactively growing M. tuberculosis cultures in 12B medium, GI500-799) was used to inoculate each of the BACTEC 12Bmedium vials containing the drugs. For the control vial, a 1:100dilution, made by transferring 0.1 ml of the suspension into9.9 ml of Diluting Fluid (Becton Dickinson and Company,Sparks, MD) was used. After mixing thoroughly by inverting at
Fig. 1. Multi-PCR-SSCP electrophoresis gel fragment patterns. Note: The lane
least 10 times, 0.1 ml of this dilution was used to inoculate the
MR, MI and MK represents rpoB, inhA and katG gene of H37Rv, respectively.
X. Cheng et al. / Journal of Microbiological Methods 70 (2007) 301–305
RIF. All of the 12B medium vials used in the test were pre-tested on a BACTEC 460TB instrument to establish a CO2atmosphere in the vial and to screen out any vials with a GI(Growth Index) of 20 or more. Bacterial suspension (0.1 mlactively growing M. tuberculosis cultures in 12B medium, GI500-799) was used to inoculate each of the BACTEC 12Bmedium vials containing the drugs. For the control vial, a 1:100dilution, made by transferring 0.1 ml of the suspension into9.9 ml of Diluting Fluid (Becton Dickinson and Company,Sparks, MD) was used. After mixing thoroughly by inverting at
Fig. 1. Multi-PCR-SSCP electrophoresis gel fragment patterns. Note: The lane
least 10 times, 0.1 ml of this dilution was used to inoculate the
MR, MI and MK represents rpoB, inhA and katG gene of H37Rv, respectively.