Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
1,026 experimental treatments in acute stroke
Victoria E. O’Collins, B.Sci,1 Malcolm R. Macleod, MRCP, PhD,3 Geoffrey A. Donnan, MD, FRACP,2
Laura L. Horky, MD, PhD,2 Bart H. van der Worp, MD, PhD,4 and David W. Howells, PhD1
Objective: Preclinical evaluation of neuroprotectants fostered high expectations of clinical efficacy. When not matched, the question arises whether experiments are poor indicators of clinical outcome or whether the best drugs were not taken forward to clinical trial. Therefore, we endeavored to contrast experimental efficacy and scope of testing of drugs used clinically and those tested only experimentally. Methods: We identified neuroprotectants and reports of experimental efficacy via a systematic search. Controlled in vivo and in vitro experiments using functional or histological end points were selected for analysis. Relationships between outcome, drug mechanism, scope of testing, and clinical trial status were assessed statistically. Results: There was no evidence that drugs used clinically (114 drugs) were more effective experi- mentally than those tested only in animal models (912 drugs), for example, improvement in focal models averaged 31.3 ؎ 16.7% versus 24.4 ؎ 32.9%, p > 0.05, respectively. Scope of testing using Stroke Therapy Academic Industry Roundtable (STAIR) criteria was highly variable, and no relationship was found between mechanism and efficacy. Interpretation: The results question whether the most efficacious drugs are being selected for stroke clinical trials. This may partially explain the slow progress in developing treatments. Greater rigor in the conduct, reporting, and analysis of animal data will improve the transition of scientific advances from bench to bedside.
A common perception of neuroprotection research is
neity, inappropriate dose, and time window). These re-
that everything works in animals but nothing works in
views have provided a solid framework for sharpening
people. This perception has been reinforced again and
experimental and clinical trial design, but, by and
again by reports of unsuccessful or mixed outcomes in
large, they have been qualitative rather than quantita-
trials of candidate neuroprotectants in acute stroke pa-
tive in nature. Additionally, only recently has the im-
tients. If animal experiments are indeed unable to in-
pact of study design and quality been examined in re-
form clinical decision making, then serious doubts are
lation to efficacy in experimental models of stroke.8–10
raised about the utility of animal models of stroke and
We set out to examine whether it is indeed true that
about the ethics of continuing current animal experi-
everything produces neuroprotection in animals, and to
compare the experimental efficacy of those interven-
In response to this challenge, several excellent re-
tions taken forward to clinical use with that of drugs
views and commentaries have tackled the issue of the
tested only in the laboratory. A broad definition of
apparent failure to translate neuroprotection successes
neuroprotection was adopted, encompassing any agent
from the laboratory to the clinical setting (for exam-
or treatment tested in an animal model of stroke,
ples, see previously published studies2–7). Such com-
whether administered with the intent of preventing
mentaries have questioned the appropriateness of the
neuronal death, restoring blood flow, or merely inves-
experimental animals (eg, age, sex, comorbidities, com-
tigating the mechanisms of damage in stroke. Thus, of
parative anatomy, sample sizes), the stroke model (eg,
the many ways one can define neuroprotection (see Ta-
anesthesia, hypothermia, glucose, reperfusion), the out-
ble 1), primacy was given to the evaluation of the final
come measures (histology vs functional deficits and
effect of a drug on the preservation of brain function,
death), study quality (blinding, randomization), and
irrespective of intended cellular target, purpose of ad-
clinical patient selection and dosing (patient heteroge-
ministration, or clinical classification of the drug.
From the 1Neuroscience Lab, Department of Medicine, University
of Melbourne, Austin Health, Heidelberg; and 2National Stroke Re-
(www.interscience.wiley.com). DOI: 10.1002/ana.20741
search Institute, Heidelberg Heights, Australia; 3School of Molecu-lar and Clinical Medicine, University of Edinburgh, Edinburgh,
Address correspondence to Dr Howells, National Stroke Research
United Kingdom; and 4Department of Neurology, University Med-
Institute and University of Melbourne, Department of Medicine,
ical Centre Utrecht, Utrecht, The Netherlands.
Austin Health, Studley Road, Heidelberg, VIC 3084, Australia.
Received Jul 25, 2005, and in revised form Oct 10. Accepted for
2006 American Neurological Association
Published by Wiley-Liss, Inc., through Wiley Subscription Services
Table 1. Definition of a Neuroprotectant
Agent administered after acute stroke to preserve neurons, in contrast with agents that restore blood
flow (thrombolytics). Limitation: Absence of strong logical argument as to why thrombolytics should be considered a dis-crete class, whereas the neuroprotectives class should include a myriad of agents themselves withother clinical uses (eg, antidepressants, fluid replacement). Furthermore, whereas the immediate tar-get of thrombolytics might be blood flow, the ultimate effect of interest is normalization of brainfunction and behavior. The direct effect of thrombolytics on neural tissue is also attracting greaterattention.
Agent containing chemical or physical properties known to be associated with neuroprotective effects. Limitation: Such properties are generally yet to be elucidated.
Agent targeting cellular pathways that control neuronal fate to preserve brain function. Limitation: Greater understanding required regarding which cells must survive to preserve brainfunction (eg, neurons, oligodendroglia, microglia) and of how the fate of individual cells relates tothe overall survival of brain tissue. More information is also needed regarding how the preservationof processes governing the recruitment and disengagement of brain networks relates to the behaviorthought to be subserved by these networks.
Agent administered with the purpose of preserving brain function. Limitation: Drugs administered for other purposes, eg, fluid replacement, antidepressants, thrombo-lytic, may also affect the preservation of brain function.
Agent whose final effect is to preserve brain structure or function. Limitation: Nonmechanistic, empirical approach does not facilitate further drug development.
A further aim was to examine the scope of preclini-
experimental phase (experimental agents); and (3) to
cal testing to which drugs have been subjected, with a
compare the experimental neuroprotective efficacy of the
view to assessing the adequacy of our procedures for
main classes of neuroprotective agents. Because neuro-
selecting drugs to carry forward to clinical trial. Here,
protective agents were being evaluated primarily for their
scope of testing refers to the range of preclinical exper-
application to stroke, greater emphasis was placed on the
imental procedures to which an intervention has been
identification and analysis of the efficacy demonstrated
subjected (eg, range of species and stroke models in
in models of focal ischemia (rather than global ischemia
which the drug was tested). Scope of testing, together
or cell culture methods) because focal models are
with quality control within individual experiments (eg,
thought to more closely mimic human stroke.15
via blinding and randomization) form the twin pillarsof the Stroke Therapy Academic and Industry Round-
Materials and Methods
table recommendations.11 These recommendations re-
Identification of Putative Neuroprotective Drugs
late to the benchmarks for preclinical evidence that
Drugs or treatments used in experimental stroke were iden-
should be met before an experimental treatment is con-
tified by (1) PubMed search for “neuroprotection”; (2)
sidered for clinical trial and represent an important
PubMed search for “cerebral ischemia” from 1960 to 1980
consensus on preclinical standards reached between
(to capture agents tested prior to the use of the keyword
several distinguished researchers in the field of stroke.
“neuroprotection”), (3) search of the test and reference lists
Neuronal injury in stroke is thought to result from a
of articles identified by (1) and (2). Drugs used in clinical
surge in activation of interlinking pathophysiological
stroke were identified by searching of clinical trial data-
pathways, with different pathways possibly predomi-
bases16,17 and clinical trial reviews18,19 and from the text and
nating in the core and at the cusp of ischemic dam-
reference lists of articles identified in the methods described
age.12–14 Neuroprotective treatments in stroke typically
above. Because the focus was on whether the interventionhas been trialed in humans and not whether the clinical trial
target one or more of these mechanisms of damage;
was well conducted, reports of any trial in humans were used
hence, we have also investigated whether efficacy in ex-
to demarcate the intervention clinical trial status.
perimental stroke was substantially different in any ofthe major categories of therapeutic agents.
The main aims of the review were therefore (1) to
Reports of efficacy in experimental stroke were identified via
identify agents tested in animal neuroprotection models
PubMed and by hand-searching of relevant journals. For
and those treatments given to acute stroke patients; (2)
each drug, a PubMed search was conducted using the search
to compare the overall quality of evidence and experi-
criteria “(drug name) AND (cerebral ischemia OR stroke OR
mental efficacy of those treatments that have been given
neuroprotection).” Where no results were found, the search
to acute stroke patients (clinical treatments) and those
was repeated using only the drug name. Information on the
agent or strategies that have not progressed beyond the
physiological effects of drugs was obtained from the Merck
Table 2. Models of Cerebral Ischemia
Clip, ligation by external filament, internal filament, inflatable cuff
Microsphere, macrosphere, autologous clot, fibrin clot, polyvinyl acetate
Endothelin-1, Rose Bengal photochemical dye, arachidonic acid, adenosine 5Ј
Potassium cyanide (KCN), asphyxia, carbon dioxide, nitrogen
Clip, tourniquet, balloon compression, decapitation, ligation, intracranial pres-
Staurosporine, C2-ceramide, paclitaxel, low potassium, etoposide, tunicamycin,
serum deprivation, Bleomycin sulfate, 3-morpholinosydnonimine, SIN-1,sodium nitroprusside (SNP), S-nitroso-N-acetylpenicillamine (SNAP)
Anoxia, hypoxia, oxygen, and glucose deprivation, veratridine, sodium cya-
nide, iodoacetic acid, sodium azide (cytochrome oxidase inhibitor),endothelin-1
H2O2, iron, heme, photochemical stress, glutathione depletion, superoxide,
naphthazarin, antimycin A, rotenone, 3-morpholinosydnonimine, sodiumnitroprusside (SNP), S-nitroso-N-acetylpenicillamine (SNAP)
Index, online chemical databases, and experimental and re-
emia experiments, with the following information also ex-
view papers. Foreign language reports were included only
tracted: animal (species sex, age, comorbidities); stroke model
when published with an English abstract.
(method of induction); intervention (dose, time treatment,mode of delivery), and outcome (end point, time measured).
Information regarding focal ischemia experiments was taken
Drug efficacy studies in established in vivo and in vitro mod-
from full publications (where available) but for other exper-
els of neuroprotection were considered for inclusion (see Ta-
iment types was generally extracted from published abstracts.
ble 2). Both focal and global models of ischemia were in-
Each experiment was given a score of Ϫ1, 0, or 1 depend-
cluded, but experiments performed in nonstroke models of
ing on whether the treatment resulted in an outcome that
neuroprotection (eg, Parkinson’s disease and epilepsy) were
was significantly worse, the same, or better than that in the
excluded. In vitro models of neuroprotection designed to
control group, respectively. Where the drug had also been
model the pathophysiology of stroke were also included and
tested in focal models of ischemia and the infarct volume
typically involved the application of a toxic stimulus (eg, glu-
(IV) reported, the average level of protection (%) was also
tamate, oxygen and glucose deprivation, hydrogen peroxide)
to a neuronal culture or coculture of neurons and astrocytes,to hippocampal or cortical slices or to retinal explants. Con-
trolled experiments measuring outcome using a functional(behavioral), histological, survival, electrophysiological, or
imaging end point were retained. For focal ischemia studies,
we included only those studies reporting outcome as infarct
volume (measured histologically or by brain imaging) or a be-havioral score. For global ischemia, we included studies report-ing survival; the extent of cell death; neurobehavioral scores; or
Scoring System for Scope of Testing
normalization of electroencephalogram. In keeping with the
A scoring system was designed to measure the diversity of evi-
Stroke Therapy Academic Industry Roundtable (STAIR) rec-
dence supporting each drug, based on the STAIR recommen-
ommendations,11 reports restricted to consideration of mech-
dations. Each drug was assigned a score (0 –10) to reflect how
anism of drug action, gene expression patterns, cerebral water
widely it has been tested in preclinical models of stroke (Table
content, blood–brain barrier function, blood flow changes,
3). Although the criteria largely reflect the STAIR recommen-
and restoration of metabolism were excluded because these
dations, several departures were made; testing in nonhuman pri-
represent surrogate end points having complex relationships
mates was not included as a criterion because the superior va-
with neuronal survival and neurological impairment.
lidity of such models is not well established. Additionally,because the focus of the review was the performance of multiple
drugs over multiple experiments, the scoring system did not in-
For each study, the following information was collected: type
clude measures relating to quality control within individual ex-
of experimental model, drug or intervention, and outcome.
periments (eg, randomization and blinding) but instead focused
A more comprehensive data set was compiled for focal isch-
on the scope of testing across experimental models.
O’Collins et al: Neuroprotective Treatments
Table 3. Quality of Evidence in Experimental Stroke Scale
Focal model tested in two or more laboratories
Focal model tested in two or more species
Focal model tested in old or diseased animalsa
Focal model tested in male and female animals
Tested in temporary and permanent models of focal ischemia
Drug administered at least 1 hour after occlusion in focal model
Drug administered using at least two doses in focal model
Tested using a feasible mode of delivery (eg, not intracisternal or intraventricular,
Both behavioral and histological outcome measured
Outcome measured at 4 or more weeks after occlusion in focal models
Not given in order of priority. aDiabetic, hypertensive, aged, hyperglycemic.
Excel and Systat 11 were used to analyze the data. All means
The initial search identified 1,150 interventions; 124
are presented as mean Ϯ standard deviation (SD). A 10(drug
were excluded from further analysis: 56 because reports
mechanism) ϫ 2(clinical trial status) analysis of variance
of their effects related only to mechanism or used non-
(ANOVA) was undertaken to evaluate the effect of clinical
eligible end points, and 68 because the literature re-
trial status and mode of drug action on outcome in focal
lated to neuroprotection in models of disease other
models of ischemia. Scope of testing was analyzed separately
than stroke. This analysis therefore is based on data for
because it did not meet the assumptions for ANOVA.
1,026 candidate stroke drugs, of which 912 have been
tested in animal models only, 97 have been tested inboth animal models and clinical trials, and 17 have
Number of Neuroprotection Experiments and
been tested only in humans. For 51% of the 114 drugs
tested in humans, the first report of its clinical use was
A total of 8,516 experimental results were extracted
published before the first report of its use in a focal
from approximately 3,500 papers (published between
ischemia model of stroke, and 42% of these drugs were
1957 to 2003). Of these, 962 experimental results were
used clinically before the first report of testing in a
excluded because they related to nonstroke neuropro-
tection models; thus, the analysis is based on 7,554 ex-perimental results from models of focal ischemia
(3,867 results), global ischemia (1,546 results), and
Of the 1,026 agents, 603 (59%) had been tested in
culture (1,341 results). The 1990s showed a marked
focal ischemia models, 256 (25%) had been tested in
growth in reports of neuroprotection experimentation
both focal and global ischemia models, and 24 (2%)
(Fig 1). At the same time, there was a less marked in-
had been tested in focal, global, and cell culture mod-
crease in reports of the first clinical application of can-didate neuroprotective drugs (Fig 2). Fig 1. Neuroprotection experiments identified from publishedFig 2. First reported clinical trials of inventions in acute
els. Neuroprotective efficacy was superior to the con-
sea snail peptides.24 More than 1,000 such drugs and
trol condition in 62% of focal ischemia experimental
nonpharmacological strategies have been tested for
results, and no different or inferior to the control con-
their neuroprotective efficacy in animal models, and at
dition in 34% and 4% of cases, respectively. In global
least 114 have been administered to acute stroke pa-
ischemia models, neuroprotective efficacy was superior
tients. Efficacy in focal ischemia ranged from 94% pro-
to the control condition in 70% of experimental re-
tection to a twofold increase in damage in the inter-
sults, and no different or inferior to the control condi-
vention versus the control condition.
tion in 26% and 4% of cases, respectively. In culture
Those drugs given to acute stroke patients were not
models, neuroprotective efficacy was superior to the
distinguished by superior efficacy in animal models of
control condition in 74% of experimental results, and
focal ischemia compared with all drugs that have been
no different or inferior to the control condition in
tested only experimentally. Given that the purely ex-
perimental class of agents included drugs used to in-
Table 4 shows the analysis of animal experiment
duce comorbid disease states in animals (eg, diabetes,
data from these comparisons for those drugs tested in
inflammation), this raises the issue of whether we are
clinical trial. For each drug, the number of positive,
in fact selecting the best drugs to carry forward to clin-
neutral, and detrimental experimental outcomes are re-
ported for each of the culture, focal, and global mod-
The unremarkable experimental track records of
some drugs given to patients may be explained by sev-eral factors. Historically, less emphasis may have been
Experimental Efficacy in Focal Models of Ischemia
placed on animal experimentation, and where it was
Because ANOVA is very sensitive to extreme results,
undertaken, the outcomes used may have related to
one study using a hamster model of focal ischemia was
metabolism or blood flow rather than neuroprotection.
excluded because it showed an unusual 1,250% in-
Second, the conditions in clinical trials often fail to
crease in damage using tissue plasminogen activator (t-
replicate the conditions under which drugs have been
PA) and 2,500% increase in damage using streptoki-
found to work in animals, especially with regard to the
nase.20 The average level of neuroprotection in focal
time of administration of treatments. Attempts to de-
ischemia models was not significantly different
sign clinical trials having greater regard to the perfor-
(F[1,416] ϭ 2.684, p Ͼ 0.05) between purely experi-
mance of drugs in animal models may assist in the
mental agents (mean, 24.4%; SD, 32.9%, n ϭ 351)
translation of results. Third, more extensive animal ex-
and treatments also used clinically (mean, 31.35%; SD,
perimentation may have been undertaken only after
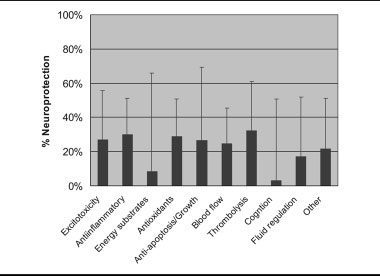
16.7%, n ϭ 66). Furthermore, the outcome in focal
clinical use in an attempt to explain negative clinical
ischemia experiments was not related to the primary
results. Finally, this review encompassed all drugs given
hypothesized mechanism of drug action (Fig 3;
to patients in the context of acute stroke with the pur-
F[9,416] ϭ 1.210, p Ͼ 0.05).
pose of improving brain function: some of these drugsmay not have been considered “neuroprotectants” in
Scope of Testing and Its Relationship to
the narrow sense, and for this reason they may not
have been tested in animal models of ischemia.
Scope of testing and its relationship to experimental
Recent developments in the formulation of guide-
efficacy was examined separately because it did not sat-
lines for design and interpretation of animal experi-
isfy the assumptions for analysis of variance. Figure 4
mentation may assist the selection of candidate drugs
shows the average level of neuroprotection (maximum
for clinical trial. Using a scale based on the STAIR
100%) versus the number of STAIR criteria satisfied
recommendations for preclinical testing, it is clear that
(maximum 10 points) for each drug. As the quality of
experimental efficacy ratings must be viewed in light of
evidence increased with more STAIR standards being
the scope of evidence supporting the use of a drug. An
met, the average level of neuroprotection of drugs
intervention should be considered for clinical trial only
tended to regress toward the overall mean of approxi-
when there is both a high level of experimental efficacy
mately 25%. Interventions tested in a broad range of
and a diverse body of evidence supporting its clinical
experimental paradigms and demonstrating a superior
application. In this review, NXY-059 and hypothermia
level of efficacy included NXY-059 and hypothermia
performed well against both these criteria, and early re-
ports from the clinical trial of NXY-059 suggest a po-tential alleviation of stroke-induced disability.25 Other
Discussion
considerations relating to cost, drug safety, regulatory
In the search for an effective treatment for stroke and
approval, intellectual property status, and putative drug
other neurological conditions, researchers have drawn
mechanism are also clearly relevant, but it may be that
from sources as diverse as Malaysian pit viper venom,21
such issues have overshadowed neuroprotective efficacy
Polynesian ceremonial beverages,22 aged garlic,23 and
O’Collins et al: Neuroprotective Treatments
Table 4. Preclinical Evidence for Drugs Administered to Acute Stroke Patients
Vascular insufficiencyImmunostimulatoryNootropic
AntioxidantReduces leukocyte activationIncreases cerebral blood flow
O’Collins et al: Neuroprotective Treatments
gen demand (CMRO2),Metabolic and synaptictransmission inhibitor.
aFirst trial ϭ the year in which the drug was first reported to have been given to acute stroke patients.
bLevel of protection ϭ average neuroprotection from infarct volume changes in focal ischemia studies.
cN ϭ number of studies from which the level of neuroprotection has been calculated
dϩ ϭ number of experimental contrasts with a significant improvement in outcome in the treatment group vs control; 0 ϭ number of
experimental contrasts showing no significant in outcome in the treatment group vs control; Ϫ ϭ Number of experimental contrasts showing
a worse outcome in the treatment group vs control.
eSTAIR quality ϭ number of STAIR criteria met by the drug (maximum 10: see Table 3).
fAnalyzed with other group because of low numbers.
No particular drug mechanism distinguished itself
Limitations: Identification of Relevant Data
on the basis of superior efficacy in animal models of
The search strategy used was broad but not deep. For
focal ischemia. This may reflect the multifaceted nature
instance, we have identified 19 publications describing
of the sequelae of ischemic stroke and suggest a role for
the efficacy of FK506 and 46 for recombinant t-PA,
combination therapy to target multiple processes. Al-
compared with 28 and 94 identified through more sys-
ternately, it might suggest that our conception of
tematic methods9 (also M. R. Macleod and colleagues,
stroke needs reformulation. A tendency to exclusively
unpublished observations). Systematic review then may
frame drug activity in terms of the dominant schema of
be combined with meta-analysis to give a more com-
stroke damage (eg. excitotoxicity, free radical damage),
plete description of the efficacy, and limits to efficacy,
coupled with the sometimes arbitrary attribution of a
for individual drugs.8,26 There is also evidence, for at
drug mechanism to one of several nonmutually exclu-
least some neuroprotectants, of a significant publica-
sive groupings, might distract from other paradigms
tion bias in favor of positive results (M.R. Macleod,
with greater explanatory power, thus hindering the de-
unpublished observations), perhaps for commercial or
velopment of more effective treatments.
other reasons. Furthermore, a strong emphasis was
is not proportional to the amount of tissue damaged,then infarct volume is compromised as a measure ofdamage.
Behavioral outcomes and neurological assessments
were not included in the quantitative aspects of thisreview. Assessment and interpretation of animal behav-ior presents additional challenges in developing strokemodels. For instance, because of the difficulties inquantifying responses to tasks, acute assessment scalesfor rats tend to rely heavily on motor effects in contrastwith clinical stroke scales. Even when nonmotor sys-tems are tested, the interpretation of the results musthave regard to potential differences between animalsand humans in terms of the importance of differentmodalities, for example, olfaction and whisker move-
Fig 3. Average neuroprotection in focal models of ischemia for
ment. For these and other reasons, animal studies tend
interventions, classified by their putative primary mode of ac-tion (100% ϭ complete protection, 0% ϭ no difference from
to place a heavy reliance upon infarct volume com-
pared with functional outcome measures more com-monly used in the clinical context.2 Nevertheless, it isrecommended that preclinical studies use both func-
placed on the identification and extraction of data
tional and histological outcomes.11 Challenges in the
from focal ischemia models because they tend to be
interpretation of behavioral outcomes are no greater
considered a better model of human stroke.11
than those encountered in understanding histologicalend points in stroke models (eg, comparative differ-
Limitations: Changing Experimental Standards
ences in gray/white matter balance, frontal lobe vol-
The scale devised for scope of testing was based on the
ume). Inclusion of behavioral outcomes in the review,
STAIR recommendations for preclinical neuroprotec-
as we have been doing in meta-analyses,8,9,26 can only
tive and restorative drug development. These recom-
assist in the understanding of experiments.
mendations were chosen as the gold standard as theyrepresent a crystallization of recent thought on animal
experimentation in stroke. Nevertheless, the reason-
A good animal model should be both reliable and
ableness of assessing past experiments using today’s
valid, that is, produce consistent, replicable outcomes,
standards may be questioned when considerable
have sound theoretical underpinnings, and have the
progress has been made in our understanding and in-
ability to predict the effect of an intervention on clin-
terpretation of animal models of stroke. Researchers’
ical outcome. The paucity of positive results in clinical
conception of the theoretical underpinnings of strokemodels has undergone much refinement over the pastdecade, and the standards for testing neuroprotectiveefficacy have been raised accordingly. Furthermore, theSTAIR standards may themselves change as moreknowledge is gained on the ability of particular modelsto predict clinical outcome. Limitations: Drug MechanismEach drug was assigned a primary hypothesized mech-anism of action. These classes were drawn broadly andmay obscure the complex and multifaceted nature ofstroke pathophysiology. Such categorization needsmuch refinement. Limitations: End PointsThe conclusions rest upon the validity of infarct vol-
Fig 4. When drugs are tested more extensively in focal models
ume as a measure of stroke damage. To the extent that
of ischemia (maximum scope of testing ϭ 10), then the aver-
different brain areas are specialized for the performance
age level of neuroprotection tends not to differ greatly from the
of different tasks, that recovery of brain function is
mean level of protection (25%). OFNE ϭ oxygenated fluoro-
plastic and that interference with learning and memory
O’Collins et al: Neuroprotective Treatments
trials, together with the disparity in clinical and exper-
V.E.O. is in receipt of an Australian Postgraduate Award scholar-
imental protocols, have hindered the validation of neu-
ship. No other funds were used to support this review process; how-
rological score and infarct volume in animal experi-
ever, G.A.D. and D.W.H. have been the recipients of industry and
ments as predictors of outcome in human disease.
government funding for research into neuroprotection.
Although animal data would support the use of NXY-
We thank D. Young and N. Spratt for their comments, and M.
059 and t-PA in the clinic, such data might also pro-
Goldberg for clarifying the status of several clinical trials.
vide tentative support for the clinical application ofmany of the other 114 therapies that have been tested
References
in humans but not undergone further clinical develop-
1. Pound P, Ebrahim S, Sandercock P, et al. Where is the evi-
dence that animal research benefits humans? Br Med J 2004;328:514 –517.
2. Gladstone DJ, Black SE, Hakim AM. Toward wisdom from
Different animal models may be needed to reflect dif-
failure: lessons from neuroprotective stroke trials and new ther-apeutic directions. Stroke 2002;33:2123–2136.
ferences in patients with acute ischemic stroke concern-
3. Cheng YD, Al-Khoury L, Zivin JA. Neuroprotection for isch-
ing stroke subtype, reperfusion status, and comorbidi-
emic stroke: two decades of success and failure. NeuroRx. 2004;
ties. Averaging across all results might mask the
potential utility of a treatment within a particular sub-
4. Green AR, Odergren T, Ashwood T. Animal models of stroke:
class of patients. For instance, thrombolytics such as
do they have value for discovering neuroprotective agents?Trends Pharmacol Sci Vol. 2003;24:402– 408.
t-PA tend to produce a better outcome in embolic
5. Grotta J. Neuroprotection is unlikely to be effective in humans
models of stroke compared with thread occlusion mod-
using current trial designs. Stroke 2002;33:306 –307.
els.27 Techniques such as meta-analysis and regression
6. Liebeskind DS, Kasner SE. Neuroprotection for ischaemic
modeling are better suited to unraveling the complexity
stroke: an unattainable goal? CNS Drugs Vol. 2001;15:
7. Del Zoppo GJ. Why do all drugs work in animals but none in
stroke patients? 1. Drugs promoting cerebral blood flow. J In-
More accurate estimates of neuroprotective efficacy will
8. Macleod MR, O’Collins T, Howells DW, Donnan GA. Pool-
be afforded through systematic review and meta-
ing of animal experimental data reveals influence of study de-
analyses for individual drugs, and this is now the focus
sign and publication bias. Stroke 2004;35:1203–1208.
9. Macleod MR, O’Collins T, Horky LL, et al. Systematic review
of the Collaborative Approach to Meta-Analysis and
and metaanalysis of the efficacy of FK506 in experimental
Review of Animal Data in Experimental Stroke, the
stroke. J Cereb Blood Flow Metab. 2005;25:713–721.
CAMARADES group. Meta-analysis and regression
10. Van der Worp HB, De Haan P, Morrema E, Kalkman CJ.
modeling of pooled data for different drugs may also
Methodological quality of animal studies on neuroprotection in
help establish whether there is indeed a “baseline” pos-
focal cerebral ischaemia. J Neurol 2005;2525:1108 –1114.
11. STAIR. Recommendations for standards regarding preclinical
itive efficacy in such studies. Further, these techniques
neuroprotective and restorative drug development. Stroke 1999;
will help elucidate the determinants of efficacy in ani-
12. Sharp FR, Lu A, Tang Y, Millhorn DE. Multiple molecular
penumbras after focal cerebral ischemia [review]. J Cereb Blood
13. Heiss W-D, Thiel A, Grond M, Graf R. Which targets are
Stroke continues to kill 5.5 million people each year,28
relevant for therapy acute ischemic stroke? Stroke 1999;30:
and the development of safe and effective treatments is
a major challenge to experimental and clinical neuro-
14. Lipton P. Ischemic cell death in brain neurons. Physiol Rev
science. The systematic review and analysis of data
from neuroprotection experiments may bring us closer
15. Hunter AJ, Mackay KB, Rogers DC. To what extent have
functional studies of ischaemia in animals been useful in the
to achieving this goal. It has been suggested that drugs
assessment of potential neuroprotective agents? Trends Pharma-
should be taken forward to clinical trial only if data
from animal experiments are valid and precise and in
16. Cochrane Central Register of Controlled Trials (CENTRAL).
the public domain before clinical trials occur1: this re-
2005. The Cochrane Collaboration, John Wiley & Sons, Ltd.
view affirms that position. Drugs taken forward to
17. Stroke Center. Clinical trials directory. Online: http://
clinical trial in the past have not been distinguished by
18. Sharma SS. Emerging neuroprotective approaches in stroke
superior efficacy in animal models, and when assessing
treatment. Current Research & Information on Pharmaceutical
experimental efficacy attention must also be given to
magnitude and scope of preclinical testing. Together
19. Labiche LA, Grotta JC. Clinical trials for cytoprotection in
with greater rigor in the conduct and reporting of an-
20. Nagai N, Vanlinthout I, Collen D. Comparative effects of tis-
imal data, there is every prospect that such an approach
sue plasminogen activator, streptokinase, and staphylokinase on
will improve the transition of scientific advances from
cerebral ischemic infarction and pulmonary clot lysis in hamster
models. Circulation 1999;100:2541–2546.
21. Huang R, Zeng J, Pei Z. [Effects of defibrinogenase on photo-
25. AstraZeneca. First results from SAINT I trial show Astra-
chemically induced middle cerebral artery occlusion in stroke-
Zeneca’s Cerovine (NXY-059) demonstrates a reduction in
prone renovascular hypertensive rats]. Zhonghua Yi Xue Za Zhi
disability in patients with acute ischemic stroke. http://
www.astrazeneca.com/pressrelease/4979.aspx, 2005.
22. Backhauss C, Krieglstein J. Extract of kava (Piper methysticum)
26. Macleod MR, O’Collins T, Horky LL, et al. Systematic review
and its methysticin constituents protect brain tissue against isch-
and meta-analysis of the efficacy of melatonin in experimental
emic damage in rodents. Eur J Pharmacol 1992;215:265–269.
stroke. J Pineal Res 2005;38:35– 41.
23. Numagami Y, Sato S, Ohnishi ST. Attenuation of rat ischemic
27. Meng W, Wang X, Asahi M, et al. Effects of tissue type plas-
brain damage by aged garlic extracts: a possible protecting
minogen activator in embolic versus mechanical models of focal
mechanism as antioxidants. Neurochem Int 1996;29:135–143.
cerebral ischemia in rats. J Cereb Blood Flow Metab 1999;19:
24. Buchan AM, Gertler SZ, Li H, et al. A selective N-type
Ca(2ϩ)-channel blocker prevents CA1 injury 24 h following
28. WHO. The World Health Report 2003. Online at
severe forebrain ischemia and reduces infarction following focal
http://www.who.int/whr/2003/en/Facts_and_Figures-en.pdf,
ischemia. J Cereb Blood Flow Metab 1994;14:903–910.
O’Collins et al: Neuroprotective Treatments
Achievements in Public Health, 1900-1999: Family Planninghttp://www.cdc.gov/mmwr/preview/mmwrhtml/mm4847a1.htm Weekly December 03, 1999 / 48(47);1073-1080 Achievements in Public Health, 1900-1999: Family Planning During the 20th century, the hallmark of family planning in the United States has been the ability to achievedesired birth spacing and family size (Figure 1). Fertility decre
Astrologi istället för professionell yrkesutövningPublicerat i Narkotikafrågan nr 3 2005 Det är svårt att komma åt de läkare som missköter förskrivningen av narkotika. Orsaken är de stränga reglerna för sekretess och integritetsskydd, som slagit över till ren dumhet. Det menade bland andra professor Edgar Borgenhammar på Svenska Carnegie Institutets seminarium om läkemedelsmis
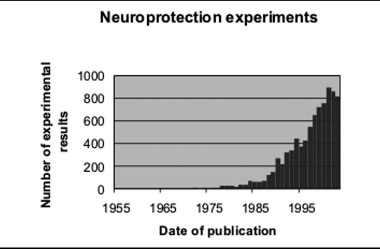
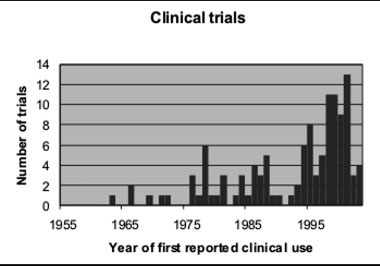 Table 3. Quality of Evidence in Experimental Stroke Scale
Focal model tested in two or more laboratories
Focal model tested in two or more species
Focal model tested in old or diseased animalsa
Focal model tested in male and female animals
Tested in temporary and permanent models of focal ischemia
Drug administered at least 1 hour after occlusion in focal model
Drug administered using at least two doses in focal model
Tested using a feasible mode of delivery (eg, not intracisternal or intraventricular,
Both behavioral and histological outcome measured
Outcome measured at 4 or more weeks after occlusion in focal models
Not given in order of priority.
Table 3. Quality of Evidence in Experimental Stroke Scale
Focal model tested in two or more laboratories
Focal model tested in two or more species
Focal model tested in old or diseased animalsa
Focal model tested in male and female animals
Tested in temporary and permanent models of focal ischemia
Drug administered at least 1 hour after occlusion in focal model
Drug administered using at least two doses in focal model
Tested using a feasible mode of delivery (eg, not intracisternal or intraventricular,
Both behavioral and histological outcome measured
Outcome measured at 4 or more weeks after occlusion in focal models
Not given in order of priority.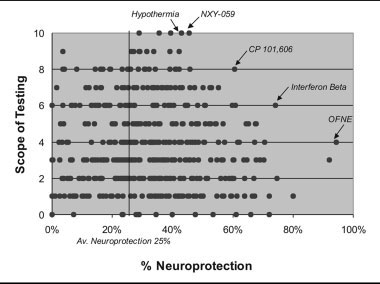
 is not proportional to the amount of tissue damaged,then infarct volume is compromised as a measure ofdamage.
is not proportional to the amount of tissue damaged,then infarct volume is compromised as a measure ofdamage.