Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Microsoft powerpoint - poster sigo
FIRST PRESENTATION Use of DermaSilk textile in recurrent vulvovaginal candidiasis MILAN, 14 – 17 NOVEMBER 2010
D’Antuono A., Bellavista S., Banzola N., Gaspari V., Patrizi A. Clinica Dermatologica - Dipartimento di Medicina Interna, Geriatria e Nefrologia – Ospedale Sant’Orsola-Malpighi - Università di Bologna INTRODUCTION MATERIAL & METHODS
Recurrent vulvovaginal candidiasis (VVC), defined as 4 or more episodes of
A randomized double-blind study versus placebo DermaSilk® versus cotton was conducted.
candida vaginitis in a year, affects about 5-8% of adult women.
In our study we have recruited 100 women of which 96 completed the study, attending to the
Pathogenesis of recurrent VVC is complex and a lot of factors influence its
Centre for Sexually Transmitted Diseases for recurrent VVC from a long period (from 1 to 6
appearance. For example, the use of tight, synthetic briefs may create a
years, mean time 2,4 years). All these patients had already been treated with weekly fluconazole
favourable environment for Candida germination. Recently, it has been
for a period exceeding 6 months with incomplete resolution, presenting recurrences and vulvar
supposed that women with recurrent VVC may develop a vaginal allergic
irritation also during treatment.
immune response towards Candida. At the recruitment, eligible patients presented an episode of acute VVC with culture of vaginal
According to the literature, the best treatment of recurrent VVC is oral
discharge positive for Candida and a vaginitis severity score ≥3 according to the evaluation
fluconazole 150 mg weekly for at least 6 months during which, in about 90% of
previously described by Sobel et al. In each patient bacterial vaginosis was excluded with pH
cases, no recurrences occur. Despite the excellent results achieved with
measurement and Gram stain microscopy.
fluconazole, it is our experience that some patients with a long history of
Women that entered the study were treated with fluconazole 150 mg for 6 months weekly. In addition, a
recurrent VVC do not reach a complete resolution during antimycotic treatment
sealed anonymous envelop, containing three pairs of DermaSilk ® briefs or white cotton briefs, was
and often require additional tools to control their symptoms. Therefore, we have decided to investigate whether underwear made of DermaSilk®, a DS GROUP: Fluconazole 150 mg + Dermasilk ® Briefs (48 patients)pure fibroin silk fabric impregnated with a permanent antimicrobial protection (AEM 5772/5), could be an additional tool in the management CT GROUP: Fluconazole 150 mg + Cotton Briefs (48 patients)of recurrent VVC, as it has been shown useful in the treatment of atopic
Patients were asked to wear only the assigned briefs for the entire period of the study. During the
dermatitis, decreasing eczema and reducing flares.
follow-up visits, after 1, 3 and 6 months, cultural examination for Candida and scoring of symptoms and
signs were repeated. A severity score ≥3 with positive culture was considered a recurrence. AIM OF THE STUDY The aim of our study was to investigate if DermaSilk® underwear may be an effective adjuvant tool in the management of recurrent VVC which has not completely responded to antimycotic treatment.
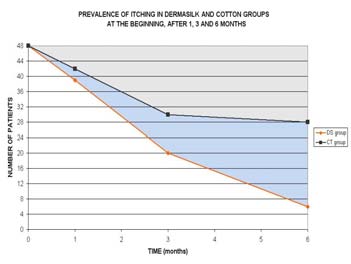
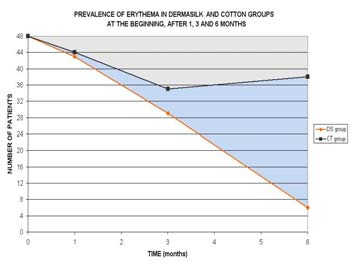
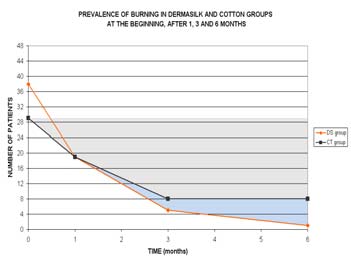
All symptoms and signs statistically improved across the whole sample. The improvement was important considering in particular erythema, itching, burning, vulvar irritation, and edema (Fisher exact test p<0,0001). PREVALENCE OF ERYTHEMA IN DERMASILK AND COTTON GROUPS PREVALENCE OF ITCHING IN DERMASILK AND COTTON GROUPS PREVALENCE OF BURNING IN DERMASILK AND COTTON GROUPS AT THE BEGINNING, AFTER 1, 3 AND 6 MONTHS AT THE BEGINNING, AFTER 1, 3 AND 6 MONTHS AT THE BEGINNING, AFTER 1, 3 AND 6 MONTHS IMPROVEMENT DUE TO DermaSilk® ACTION Comparing the two groups, at the last follow-up the DermaSilk group (DS) showed a significantly greater decrease in erythema, itching and burning than the cotton briefs (CT) group as shown in the graphs above. Recurrences: 11/48 (22,9%) patients of DS group reported NUMBER OF DS CT
no recurrences during the study, compared with only 4/48
RECURRENCES GROUP GROUP
(8,3%) patients of CT group (Fisher exact test p=0,036). Most of patients of DS group (32/48, 66.7%) had none or one recurrence; most of patients of CT group (29/48, 60.5%) had 2 recurrences or more. DISCUSSION DERMASILK® is a high technology fine-knitted fabric made of 100% pure fibroin (medical grade sericin-free silk) impregnated with a non-migrating permanent antimicrobial protective finish (AEM 5772/5)
-DermaSilk is considered an effective adjunctive therapy in the management of atopic dermatitis and had been included in the latest European guidelines for atopic dermatitis
-in vitro studies demonstrated that DermaSilk induces a significant decrease in S.Aureus, Pseudomonas aeruginosa and Candida albicans levels
-in the present study, the use of DermaSilk briefs generated statistically better results in reducing itching, burning and erythema, compared to cotton briefs in a group of patients with a history of recurrent VVC which has been previously treated with long term antimicotic treatment with incomplete response
-the study shows that the use of DermaSilk briefs diminished the number of recurrences of VVC during antimycotic treatment compared with cotton briefs DERMASILK ®
• decreases external sources of vulvar irritation
• absorbs sweat maintaining a good water balance in vulvar mucosa
• does not exacerbate the immuno-mediated inflammatory processes already present in many women
• hygroscopic and heat regulating properties
+ Antimicrobial agent (AEM 5772/5)
• aims to restore the skin barrier function, altered by inflammation, irritation and infections
• in vitro is able to decrease Candida contamination
DermaSilk® briefs appear to be an adjuvant tool, free of side effects, that can be added to classical antimycotic treatment in difficult patients in order to diminishing vulvar discomfort and reduce recurrences of VVC.
Sobel JD. Vulvovaginal candidosis. Lancet 2007; 369:1961-71.
Weissanbacher TM, Witkin SS, Gingelmaier A, Scholz C, Friese K, Mylonas I. Relationship between recurrent vulvovaginal candidosis and immune mediators in vaginal fluid. Eur J Obstetr Gynecol 2009; 144:59-63.
Senti G, Steinmann LS, Fischer B, Kurmann R, Storni T, Johansen P, Schmid-Grendelmeier P, Wuthrich B, Kundig TM. Antimicrobial silk clothing in the treatment of atopic dermatitis proves comparable to topical
corticosteroid treatment. Dermatology 2006; 213:228-233
Darsow U, Wollenberg A, Simon D, Taieb A, Werfel T, Oranje A, Gelmetti C, Syensson A, Deleuran M, Calza AM, Giusti F,Lubbe J, Seidenari S, Ring J. European Task Force on Atopic Dermatitis. EADV Eczema Task
Force. ETFAD/EADV eczema task force 2009 position paper on diagnosis and treatment of atopic dermatitis. J Eur Acad Dermatol Venereol 2010 Mar; 24(3): 317-28.
Haug S Roll A, Schmid-Grendelmeier P, Johansen P, Wüthrich B, Kündig TM, Senti G. Coated textiles in the treatment of atopic dermatitis. Curr Probl Dermatol 2006; 33:144-151.
2005-2006 Field Guide to Antibiotic Therapy I N T R O D U C T I O N Proper antibiotic selection requires a knowledge of hostrosyphilis because of limited penetration into the centralfactors (e.g., immune function, comorbid diseases, andnervous system. Similarly, cefotaxime has activity againstage);
Management of Complex Ovarian Cysts in Women with Management of Complex Ovarian Cysts in women with Postmenopausal Bleeding Abstract Introduction : Transvaginal ultrasound (TVS) to determine endometrial thickness is recommended in women with postmenopausal bleeding (PMB). TVS may also detect extra-endometrial pathology including ovarian cysts. National guidelines exist regarding ma


 FIRST PRESENTATION
FIRST PRESENTATION