Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Microsoft word - kalp5.doc
Intermittent Shear Stimuli by Enhanced External Counterpulsation (EECP) Restores Endothelial Function in Patients with Coronary Artery Diseases. Urano, H, Circulation 102:18 Suppl. II Oct. '00
"As goes the endothelium, so goes the patient" is a scientifically correct statement. The endothelium refers to the thin layer
of cells that line our arteries and veins. These cells are essentially tiny hormone and angiochemical producing factories.
They make the "good guys", nitric oxide and VEGF, which promote vascular wall integrity, blood vessel vasodilation, and the
growth of new vessels. The endothelium also makes "bad guys", such as endothelin, which promotes vasoconstriction,
abnormal clotting, and plaque deposition. Endothelial health determines whether the good guys or bad guy angiochemicals
will dominate, and has been shown to be a key indicator of cardiovascular health and long-term outcome. We can
accurately assess endothelial health by measuring brachial artery flow mediated vasodilation. Here we measure the
diameter of the brachial artery (the major artery to the arm at the level of the elbow), before and after release of a blood
pressure cuff, which had been inflated enough to impair flow to the forearm for five minutes. As blood flow is restored to the
forearm, the brachial artery will dilate by 10-12% to accommodate this increased flow, if endothelial function is normal. If
endothelial function is mildly impaired, flow mediated vasodilation will be less than 10%. In patients with established
cardiovascular disease, or risk factors for cardiovascular disease such as hypertension, smoking, or high levels of
homocysteine or LDL cholesterol, endothelial function may be severely impaired, and the brachial artery will actually
constrict. Indeed, endothelial dysfunction may be a final common pathway through which many of the causes or
cardiovascular disease actually cause cardiovascular disease. Multiple studies have shown that the health of the
endothelium at a given point in time is a critical determinant of the cardiovascular health and vital status of the patient 2 to 5
years later. Whether we are looking at patients with angiographically normal coronary arteries and spasm, individuals with
non-obstructive atherosclerosis, or patients with obstructive multi-vessel disease, those with preserved endothelial function
do well, while those with impaired endothelial function at baseline are at increased risk for a future adverse cardiac event.
The worse the endothelial function, the greater the likelihood that an event will occur. So far, treatments that improve
endothelial function have been shown to improve outcome. Accupril, a prescription agent, improves endothelial function by
blocking endothelial bound ACE, a nitric oxide degrader. Accupril decreases restenosis after angioplasty or stent
placement, and the QUO VATUS study showed us that Accupril decreases one-year post-CABG event rate by 80%.
Vitamin E blocks endothelial superoxide, another nitric oxide degrader; the CHAOS study demonstrated that vitamin E,
begun after angiography, reduced two year event infarction/death rate by 47%. During exercise blood flow velocity and
quantity increase, exerting a radial shearing stress on the endothelium. A healthy endothelium, and to a somewhat lesser
extent an unhealthy endothelium, will respond by elaborating more nitric oxide. Nitric oxide will in turn improve endothelial
function, dilating the vessel to accommodate the increased flow, and will promote collateral generation. Exercise leads to an
increase in nitric oxide and multiple studies have shown that regular exercise improves outcome – this is why cardiac rehab
EECP certainly improves the outcome of coronary patients, and EECP certainly increases the velocity and quantity of blood
flow, not just in the coronaries but also within every vascular bed in the body. We know that EECP increases nitric oxide
and VEGF and decreases endothelin levels, so the logical question is – Can EECP improve endothelial function?
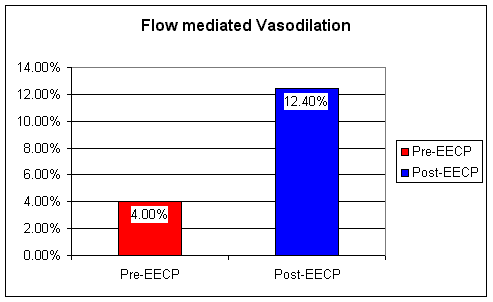
To answer this question, Urano measured flow mediated brachial artery vasodilation, a reproducible, accurate measure of
systemic and coronary endothelial function, before and after a 35-hour course of EECP, given to stable angina patients with
documented coronary disease and abnormal stress EKG studies. The patients' clinical status and treadmill findings
improved, consistent with all prior studies.
Flow mediated brachial artery vasodilation, significantly impaired at baseline at 4%, improved 3-fold following EECP to 12%,
essentially a normal value. It's becoming clear that EECP decreases symptoms and improves outcome not just by forcing
open collaterals, but also by improving the patient's biochemistry and endothelial function. It hasn't been studied yet, but it is
my impression that measures designed to improve endothelial function, such as tissue specific ACE inhibitors, arginine,
omega-3 essential fatty acids, and anti-oxidants, improve and extend the patient's response to external counterpulsation.
These agents all have beneficial effects on their own, so now I typically place new EECP patients on an "endothelial
cocktail" of these treatments, and continue it post-EECP.
10a. Endothelial function in patients with severe coronary artery disease treated with enhanced external counterpulsation (ECPT). Schechter, M, et al. European Heart Journal (2002) 23 (Abstract Supplement) - P2363, page 463.
Urano's study, abstracted above, demonstrates that EECP restores endothelial function in patients with coronary
insufficiency, certainly a good thing; his study was carried out in Japan. In this paper, Schechter and colleagues repeat
Urano's study, here in an Israeli population of inoperable coronary patients with persistent class 3 to 4 symptoms. Their
normal range was not given, and may be different from Urano's (different researchers may use different measuring
techniques so their "normal" values may be different), but in Schecter's population, just as in Urano's, percent flow mediated
vasodilation, the measure of endothelial tone, increased with external counterpulsation, here from 3.5 to 8.2%, coincident
with a reduction in average NTG need from 4.7 to 0.4 tabs per day, and an improvement in functional class from 3.3 to
2.0. No matter which continent you use it in, or what you call it (EECP in the US, Asia, and Europe or ECPT in Israel),
external counterpulsation works. Endothelial function, the critical predictor of cardiovascular health and outlook, improves,
while previously treatment refractory symptoms recede or resolve.
Pneumatic External Counterpulsation: A New Noninvasive Method to Improve Organ Perfusion. Werner, D, The American Journal of Cardiology 1999;84:950-52
In China, EECP is not confined to the treatment of coronary insufficiency. Stroke, cerebrovascular insufficiency, hepatitis,
and even diabetes have been addressed with external counterpulsation with measurable benefits. Why should this be? We
know that all of these disease states involve free radical tissue damage. Dr.Quan, in article 7, is going to show us that
EECP has a significant antioxidant effect. EECP increases blood flow to the coronary arteries that serve the heart. Could
an increase in blood flow, with an attendant increase in oxygen and fuel supply to the diseased organ be a mechanism of
benefit? Werner and colleagues set out to measure the effect of EECP on blood flow to different organ systems. They used
doppler ultrasound (as in Dr. Katz's study - article 1) to measure blood flow per heart beat at rest, during EECP using calf
and thigh cuff inflation, and during EECP using calf, thigh, and lower abdominal/pelvic cuff inflation (the method we use in
300 mm Hg - calves, thighs, & pelvis
EECP increases blood flow everywhere, not just to the heart. Organ dysfunction present on the basis of reduced blood flow
could thus improve during EECP. In China, arm cuffs are utilized, further increasing blood flow to the brain, and in this
fashion EECP is used in the treatment of stroke. This ability of EECP to improve blood flow in general may lead to some
additional applications of EECP in this country - research is ongoing and much more is planned
Every euro counts these days so what savings can you make on the health front? – Here are a few ‘savings savvy’ ideas. Don’t be afraid to ask for generic alternatives of over the counter drugs,” says Irish Pharmacy Union spokesperson Kathy Maher. “Also ask your doctor to prescribe generically rather than write Amy Bracken meets a group of rural women brand names down on
Geriatric depression is associated with disability, a dramatic increase in the rate of completed suicide, higher mortality in the medically ill elderly, and greater risk of Alzheimer’s dementia (AD). Depression in the elderly is a clinically and neurobiologically heterogeneous disorder.The clinical management of geriatric depression is complicated by age- related changes in cognition and neu
 Flow mediated brachial artery vasodilation, significantly impaired at baseline at 4%, improved 3-fold following EECP to 12%,
essentially a normal value. It's becoming clear that EECP decreases symptoms and improves outcome not just by forcing
open collaterals, but also by improving the patient's biochemistry and endothelial function. It hasn't been studied yet, but it is
my impression that measures designed to improve endothelial function, such as tissue specific ACE inhibitors, arginine,
omega-3 essential fatty acids, and anti-oxidants, improve and extend the patient's response to external counterpulsation.
These agents all have beneficial effects on their own, so now I typically place new EECP patients on an "endothelial
cocktail" of these treatments, and continue it post-EECP.
10a. Endothelial function in patients with severe coronary artery disease treated with enhanced external
Flow mediated brachial artery vasodilation, significantly impaired at baseline at 4%, improved 3-fold following EECP to 12%,
essentially a normal value. It's becoming clear that EECP decreases symptoms and improves outcome not just by forcing
open collaterals, but also by improving the patient's biochemistry and endothelial function. It hasn't been studied yet, but it is
my impression that measures designed to improve endothelial function, such as tissue specific ACE inhibitors, arginine,
omega-3 essential fatty acids, and anti-oxidants, improve and extend the patient's response to external counterpulsation.
These agents all have beneficial effects on their own, so now I typically place new EECP patients on an "endothelial
cocktail" of these treatments, and continue it post-EECP.
10a. Endothelial function in patients with severe coronary artery disease treated with enhanced external