E. M. C. Passaro, M. T. Silveira and N. Y. S. Valente
Department of Dermatology, Hospital do Servidor Pu´blico do Estado de Sa˜o Paulo, Brazil
Follicular mucinosis is a rare chronic inflammatory disease of unknown aetiology,
presenting as mucin deposits around the follicles and sebaceous glands. It can progressto alopecia of the scalp and other hairy areas. Follicular mucinosis may be a benignprimary idiopathic disorder or secondary to malignant lymphoproliferative disorders. Itcan present with shiny papules or sharply marginated infiltrated erythematous scalingplaques, with follicular accentuation on the scalp, neck, trunk and limbs. There aremany local and systemic treatments. This paper discusses the case of an adult with anuncommon acneiform follicular mucinosis controlled with systemic corticosteroids.
lymphoproliferative processes such as cutaneous T-
and B-cell lymphomas, Hodgkin’s disease, chronic and
acute lymphocytic leukaemia.1 Two categories of dis-
mucinosis in 1957 under the term alopecia mucinosis,
ease have been identified in patients with the benign
which was given in reference to a disease process of
primary form. The first occurs in younger patients: there
follicular degeneration resulting in alopecia. Histologi-
are few lesions limited to the head and neck or upper
cally the process manifests as deposition of mucin in the
arms and which disappear spontaneously between
epithelium of the follicular outer root sheath and
2 months and 2 years after onset. The second is a
sebaceous glands.1 The condition was later renamed
disorder of adult patients: the lesions are larger and
follicular mucinosis by Jablonska, Chorzelski and
more widespread and can take a longer period to
Lancucki in 1959 because alopecia is not always
improve. In the second type, which is linked to
malignant lymphoproliferative conditions, the patients
Follicular mucinosis is a chronic inflammatory disease
are older and have widespread and infiltrated lesions
of unknown aetiology. It is more commonly observed as
that can progress to mycosis fungoides (MF).1,2
shiny pink or pale-coloured follicular papules or as
The origin of the mucin deposits in the follicles is
erythematous scaling infiltrated plaques. The involved
unknown, but immunopathological studies have shown
follicles may show conspicuous horny plugs, presenting
that cytokines released from perifollicular T lympho-
with alopecia when the scalp or other hairy regions are
cytes might stimulate the follicular epithelium to secrete
involved. The lesions may be localized or widely
mucin.3,4 Immunohistochemical studies have shown
disseminated. There are various distinctive clinical
expansion of clonal T cells in many cases of primary
presentations: alopecia areata-like, scarring alopecia,
‘benign’ mucinosis. The clonality is not always synony-
nodules, cysts, chronic eczema and acneiform eruption.1
mous with malignancy, but its presence is a reason for
primary disorder or be associated with malignant
Various therapies have been tried for follicular muci-
nosis: indomethacin, topical and systemic corticosteroids,dapsone, topical tretinoin, oral isotretinoin, minocycline,
Correspondence: R. M. C. Passaro, R. Joa˜o de Souza Dias, 509 ⁄ 122, CampoBelo-Sa˜o Paulo, Brazil, 04618
tetracycline and psoralen with ultraviolet A.3,6 When the
Tel.: +55 11 5088 8293. Fax: +55 11 5088 8293
condition has been associated with lymphoma, radio-
therapy, topical nitrogen mustard, electron beam radi-
ation and immunotherapy have been tried.7
Ó 2004 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 29, 396–398
Acneiform follicular mucinosis • E. M. C. Passaro et al.
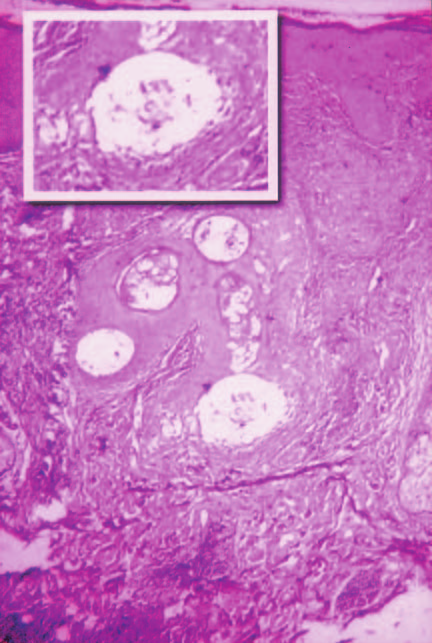
Figure 2 Histopathology shows, in the centre of the field, a folliclesurrounded by a mixed inflammatory infiltrate. Mucin depositscan be seen in the outer sheath of the follicle (highlighted in thefigure inset). (Haematoxylin & eosin).
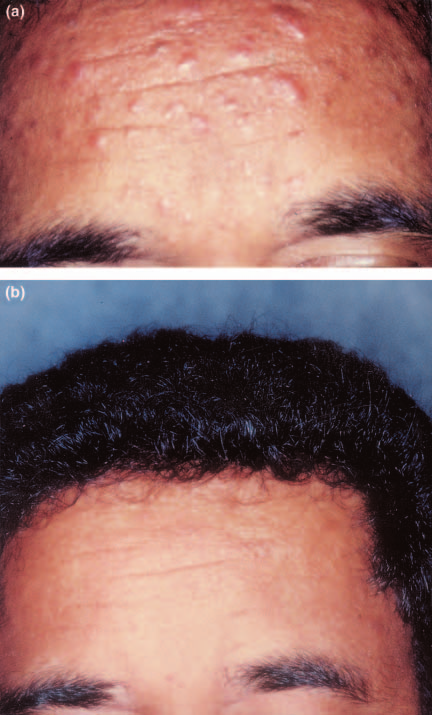
Figure 1 (a) Multiple erythematous follicular papules and noduleson the forehead and temples before treatment. The papules arenot coalescent and present an acne-like aspect. (b) Completeregression of the cutaneous lesions following treatment with oralprednisone 40 mg ⁄ day.
surrounding the hair follicles. A few eosinophils werepresent. Special stains for fungi and acid-fast bacilliwere negative. Demodex folliculorum was not isolated.
We report the case of a black 36-year-old male
Syphilis and HIV serology were negative. Rosacea was
patient, who complained of nodules on his face with
the most likely diagnosis and so tetracycline, 1.5 g per
slight pruritus that increased after sun exposure. The
day, was given for 30 days but the patient did not
lesions first became apparent 1 year before presentation.
Physical examination showed multiple red or pale
A second biopsy revealed an inflammatory infiltrate
isolated papules and nodules on his forehead (Fig. 1a),
around the follicles composed of lymphocytes, histio-
temples and behind his ear, without lymphadenopathy.
cytes and moderate number of eosinophils. Follicular
The patient had no history of acne. At that time the
epithelium showed cystic holes provoked by intracellu-
diagnostic possibilities included: granulomatous rosa-
lar and intercellular oedema (Fig. 2). Deposition of
cea, demodicidosis, cutaneous tuberculosis, sarcoidosis,
mucin in the follicular epithelium was demonstrated by
Jessner–Kanof lymphocytic infiltrate, lupus erythema-
Alcian blue stain. These findings confirmed the diagno-
tosus, lymphocytoma cutis, lymphoma and syphilis.
sis of acneiform follicular mucinosis. Laboratory exam-
Histopathological examination showed deep and
ination revealed a normal full blood count, renal and
superficial dermatitis with an inflammatory infiltrate
liver function tests and chest X-ray.
Ó 2004 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 29, 396–398
Acneiform follicular mucinosis • E. M. C. Passaro et al.
We decided to treat the patient with oral predni-
sone, 40 mg ⁄ day for 20 days. The patient improvedquickly and the lesions disappeared entirely (Fig. 1b).
The authors thank Prof Dr Cidia Vasconcellos, Dr Paulo
Prednisone was gradually decreased by 10 mg weekly
Ricardo Criado and Dr Mario Cesar Pires, Department of
and was discontinued after 48 days. The patient has
been followed up carefully for 7 months without
Sa˜o Paulo, for their helpful comments.
Deposits of mucin in the follicles have been described in
various dermatoses: alopecia areata,1,5 lichen planus,5melanocytic nevus,1,8 lentigo maligna,8 sarcoidosis,5
1 Bonta MD, Tannous ZS, Demierre MF et al Rapidly
squamous cell carcinoma,9 lupus erythematosus,1,5,7,10
progressing mycosis fungoides presenting as follicular
arthropod bites,1,4,5 pseudolymphoma5 and Hodgkin’s
mucinosis. J Am Acad Dermatol 2000; 43: 635–40.
disease.5,11 Some authors have described follicular
2 Pereyo NG, Requena L, Galloway J et al Follicular mycosis
fungoides: a clinicohistopathologic study. J Am Acad
mucinosis with an acneiform clinical presentation1,3
but this raises the question of whether the deposition of
3 Wittenberg GP, Gibson LE, Pittelkow MR et al Follicular
mucin around the follicles is primary or secondary.
mucinosis presenting as an acneiform eruption: report of
We consider that further studies are necessary to clarify
four cases. J Am Acad Dermatol 1998; 38: 849–51.
4 Abajo P, Martı´n R, Daude´n E. Follicular mucinosis associ-
When the infiltrated lesions are generalized with a
ated with cutaneous leishmaniasis. Acta Derm Venereol
chronic course in patients over 30 years old the risk of
association with MF is high. Histopathological features
5 Jackow CM, Papadopoulos E, Nelson B et al Follicular
that draw attention to this include the presence of
mucinosis associated with scarring alopecia, oligoclonal
atypical lymphocytes, epidermotropism and a paucity of
T-cell receptor Va expansion, and Staphylococcus aureus:
eosinophils. However, there are reports of follicular
when does follicular mucinosis become mycosis fungoides?J Am Acad Dermatol 1997; 37: 828–31.
mucinosis that progressed to MF in children or in
6 Yotsumoto S, Uchimiya H, Kanzaki T. A case of follicular
patients with only a few isolated lesions on the face and
mucinosis treated successfully with minocycline. Br J
neck.1 Some authors have observed that MF associated
with, or preceded by, follicular mucinosis is more
7 Klemke CD, Dippel E, Assaf C et al Follicular mycosis
aggressive with lymph node involvement; histopatho-
fungoides. Br J Dermatol 1999; 141: 137–40.
logical examination shows folliculotropism without
8 Summer WT, Grichnik JM, Shea CR et al Follicular muci-
epidermotropism, i.e. follicular MF.2 The folliculotropic
nosis as a presenting sign of acute myeloblastic leukemia.
variant of MF may require aggressive and distinct
J Am Acad Dermatol 1998; 38: 803–5.
modalities of treatment because 7% of cases progress
9 Walchner M, Messer G, Rust A et al Follicular mucinosis in
rapidly to lymph node involvement as compared with
association with squamous cell carcinoma of the tongue.
less than 3% of classic MF cases.1,7 At present the
J Am Acad Dermatol 1998; 38: 622–4.
10 Dawn G, Handa S, Kumar B. Follicular mucinosis and
treatment options are electron beam radiation, immu-
systemic lupus erythematosus. Dermatology 1997; 195:
Patients with follicular mucinosis, whether children
11 von Kobyletzki G, Kreuter JA, Nordmeier R et al Treatment
or adults, presenting with uncommon clinical variants
of idiopathic mucinosis follicularis with UVA1 cold light
must be followed up clinically and histologically to
phototherapy. Dermatology 2000; 201: 76–7.
detect any evolution into cutaneous lymphoma.
Ó 2004 Blackwell Publishing Ltd • Clinical and Experimental Dermatology, 29, 396–398
Medical data is for informational purposes only. You should always consult your family physician, or one of our referral physicians prior to treatment. tients from angina, claudication, and dizziness. However with longterm and extensive use the benefits of chelates are lost with thenonspecific removal and reduction of the essential trace metals. Chelation therapy can be a double edge sword li
Objet : Convocation à l’assemblée générale mixte Cher adhérent, chère adhérente, La Fédération Addiction vous convoque à son assemblée générale mixte. Cette assemblée générale est précédée d’un débat de pré AG sur le thème « Place du médicament dans le soin et l’accompagnement aujourd’hui : suboxone et baclofène ? » Elle aura lieu le Mercredi
 Acneiform follicular mucinosis • E. M. C. Passaro et al.
Acneiform follicular mucinosis • E. M. C. Passaro et al.