Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
No job name
The Clinical Respiratory Journal Sexual function in male patients with obstructive sleep apnoeacrj_1731.6
Marian Petersen1,2, Ellids Kristensen3,4, Søren Berg2,5,6 and Bengt Midgren1,2
1 Department of Respiratory Medicine, Lund University, Lund University Hospital, Lund, Sweden2 Lund Sleep Study Group, Lund University, Lund University Hospital, Lund, Sweden3 Sexological Clinic, Psychiatric Centre Rigshospitalet, University Hospital of Copenhagen, Copenhagen, Denmark4 Department of Neurology, Psychiatry and Sensory Sciences, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark5 Department of ENT, Head and Neck Cancer, Lund University, Lund University Hospital, Lund, Sweden6 ScanSleep, Copenhagen, Aalborg, Aarhus, Denmark
Abstract Key words Objective: Our objective was to investigate general and functional aspects of sexu-
male – obstructive sleep apnoea –
ality in male patients with a confirmed diagnosis of obstructive sleep apnoea (OSA)
and compare the results with normative data. Correspondence Materials and Methods: We investigated 308 male patients (age 30–69) admitted to
a sleep laboratory and receiving a diagnosis of OSA, using questions drawn from
Respiratory Medicine, University Hospital of
two self-administered questionnaires on sexuality [Fugl-Meyer Life satisfaction
checklist (LiSat) and Brief Sexual Function Inventory (BSFI)]. Results: We found that both general (Fugl-Meyer LiSat) and functional (BSFI)
aspects of sexuality were worse in patients with (untreated) OSA when compared
with normative data. Both aspects were dependent on age, obesity, social factors
and concomitant medication but not on the severity of OSA as reflected by the
apnoea–hypopnoea index or subjective sleepiness. Conclusion: We conclude that although sexual dysfunction is more prevalent inOSA patients than in the general population, it is a complex problem relating more
to age, obesity, social factors and comorbidity than to the severity of OSA. Authorship Marian Petersen initiated, designed and
Please cite this paper as: Petersen M, Kristensen E, Berg S, Midgren B. Sexual
performed the study, collected and analysed
function in male patients with obstructive sleep apnoea. The Clinical RespiratoryJournal 2009; DOI:10.1111/j.1752-699X.2009.00173.x.
Kristensen contributed to the design, analysedthe data and wrote the paper. Søren Bergcollected and co-analysed the data and wrotethe paper. Bengt Midgren supervised theanalysis of data and the writing of the paper. Ethics Informed consent was obtained, and the study was reviewed and approved by the Ethical Committee of Copenhagen. Conflict of interest Marian Petersen has received an unconditioned research grant from Maribo Medico. Ellids Kristensen has no conflicts of interest. Søren Berg is one of the owners and managers of ScanSleep; otherwise he has no conflicts of interest. Bengt Midgren has received payment from ResMed Sweden for lectures and consultant commitments.
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
Introduction
field, CO, USA). The recording montage includednasal airflow using a nasal pressure catheter, respira-
Obstructive sleep apnoea (OSA) is characterized by
tory movement with thoracic and abdominal bands
repetitive cessation of breathing during sleep due to
(XactTrace, Embla, Broomfield, CO, USA), pulse
upper airway collapse. When this is associated with
oximetry and body position. Apnoeas were diagnosed
daytime sleepiness it is termed obstructive sleep
as cessation of breathing more than 10 s. Hypopnoeas
apnoea syndrome (OSAS). With regard to the effects of
were diagnosed as reduction in airflow >40% associ-
OSA on sexuality, different aspects have been investi-
ated with a desaturation of 4% or more. The number
gated. Sexuality has been reported to be affected by
of apnoeas and hypopnoeas/hour (AHI) was calcu-
decreased hormonal production (1), low sexual drive
lated on estimated sleep time (as reported by the
and satisfaction and decreased morning erection (2).
These effects may lead to misconceptions by the
Data of self-reported daytime sleepiness were col-
patient with regard to his or her relationship and
lected using the Epworth Sleepiness Scale (ESS). The
potentially lead to feelings of fault, blame and guilt,
ESS assesses the likelihood of the patient dozing off or
which may further negatively affect the relationship
falling asleep in eight daily situations using a score
(3). Erectile dysfunction is estimated to be present in
between 0 and 3. The maximum score is thus 24, with
30% of untreated OSAS patients (4). O’Leary et al.
a score of 11 or more being taken to indicate significant
found that age is a main factor for erectile dysfunction
levels of daytime sleepiness (7). ESS data were collected
in a normative sample of men, but that sexual desire is
from only 192 patients because of a late change of
maintained in later years (5). Other studies have high-
lighted the correlation between high respiratory dis-
Data on sexual function were obtained using two
turbance index and erectile dysfunction (2).
self-administered questionnaires. One was the Fugl-
Most previous studies of the effects of OSA on sexu-
Meyer Life satisfaction checklist (LiSat) (8), from
ality in men have focused on erectile dysfunction. One
which we selected four questions concerning general
of the few other studies in this area was reported by
satisfaction with life: Life as a Whole and three
Hanak et al. (6). However, their study investigated only
domains of closeness (Sexual Life, Partner Relation-
elderly snorers (51–90 years) and their risk for sexual
ship, Family Life). The referent population consisted of
dysfunction. We therefore designed this study to inves-
both sexes, but we used data on male only received
tigate general and functional aspects of sexuality in
from Fugl-Meyer (A. Fugl-Meyer, pers. comm.). Satis-
male patients with untreated OSA and to compare
faction was scored on a scale from 1 to 6, with higher
these findings with normative data. We have per-
scores indicating greater satisfaction. The other ques-
formed a similar study on females with OSA (to be
tionnaire was the Brief Sexual Function Inventory
published), and follow-up studies (for both sexes) after
(BSFI) (9) in which the first 10 items cover functional
1 year on continuous positive airway pressure (CPAP)
aspects of male sexuality during the past 30 days:
Sexual drive and level of sexual drive (two items),partial or full erection, capability to intercourse anddifficulties in getting erection (three items), difficulty
Material and methods
ejaculating and satisfaction with the amount of semen(two items) and problem assessment concerning
Male patients with OSA were consecutively recruited
sexual drive, erection and ejaculation (three items).
from patients assessed in three sleep laboratories of
The last item covers overall sexual satisfaction and con-
one sleep clinic (ScanSleep) in Denmark from October
sists of one question. The items were scored from 0 to
2005 to January 2008. The study comprised only
4, with higher scores indicating better function. The
patients more than 18 years old, able to read and write
total score was calculated for the first 10 items. Item 11
Danish and with a diagnosis of OSA [apnoea–
(overall satisfaction) is not a functional question and
hypopnoea index (AHI) >5] requiring treatment with
was therefore analysed separately, and not included in
CPAP. The material thus consisted only of patients
the statistical analyses for total score.
where CPAP was considered as being the clinically rel-
Socio-demographic data on age, body mass index
evant treatment of choice as judged by an experienced
(BMI), marital status and education were collected for
specialist. Approximately 90% of the eligible patients
all individuals, and their current use of medication was
recorded as a proxy for comorbidity. No control data
All patients were investigated for OSA using identi-
on Fugl-Meyer LiSat or on BSFI has been reported for
cal portable devices (EMBLETTA®, Embla, Broom-
the Danish population. We therefore used normative
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
Table 1. Clinical and demographic characteristics of obstructive sleep apnoea male patients according to age
*Digoxin, antihypertensive, diuretics, beta blockers, calcium antagonists, ACE inhibitors. †Anti-psychotics, anxiolytics, antidepressants. BMI, body mass index (kg/m2); AHI, Apnoea Hypopnoea Index; ESS, Epworth Sleepiness Scale.
male data from Sweden and Norway since they are
BMI was 31.5 (SD = 6.3) and AHI was 39.9 (SD = 24.2)
countries linguistically, culturally and sociologically
for the selected age groups. The mean score for ESS was
closely related to Denmark. From Sweden, Fugl-Meyer
11.5 (SD = 4.0). Socio-demographic data for OSA
LiSat-11 data were collected by questionnaires and
patients showed that 84% lived with a partner, 54%
face-to-face interviews, and participants were drawn
had 10 or more years of education and 77% were
from the Swedish Central Population Register (8) and
employed. Ninety-two (29.9%) patients received
from Norway (for BSFI) participants were recruited by
medication for cardiovascular reasons. Thirty-three
using public address lists and sending questionnaires
(10.7%) received psychopharmaca and 20 (6.5%) were
receiving treatment for diabetes. Data for age groups
Statistical analysis was performed with SPSS (version
15.0 for Windows). Descriptive statistics [mean andstandard deviation (SD)] were used to summarize theclinical and socio-demographic data. A power analysis
Fugl-Meyer LiSat
with respect to the 6-point scale Fugl-Meyer LiSat
Scores on Life as a Whole were significantly lower in
showed that 80 patients would be sufficient to demon-
all OSA patients than in the control group (Table 2).
strate with 95% certainty a difference between normals
For Family Life, the groups of 40–49 and 50–59 years
and patients of 0.5 points at the 0.05 one-side signifi-
scored significantly lower than the control group.
cance level, assuming that the patients had the same SD
Regarding Partner Relationship, only the group of
as the normal subjects. Regression analysis was per-
50–59 scored lower than the control group, and for
formed for the Fugl-Meyer LiSat and BSFI, to assess the
Sexual Life, the age groups 40–49, 50–59 and 60–69
specific impact of BMI, AHI, ESS, being in a relation-
scored significantly lower than controls. To assess the
ship, education, employment and medication. T-tests
specific impact on OSA patients of BMI, AHI, ESS,
were used when comparing study data with reference
having a relationship, education, employment and
subjects based on available data for n and SD. A sig-
medication, a regression analysis was performed for
nificance level of P Յ 0.05 was used for all statistical
each of the four items: Life as a Whole, Family
Life, Partner Relationship and Sexual Life. Lifeas a Whole was significantly negatively associated
with age (P = 0.005), with cardiovascular medication(P = 0.012) and with psychopharmaca (P = 0.001).
Three hundred fifteen male patients aged 26–77 years
No association with BMI, AHI, ESS, having a rela-
(mean 50.6, SD 10.3) were included in the study.
tionship, education, employment or diabetes was
Because of the low number of OSA patients in age
found. For Family Life, being in a relationship had a
groups 20–29 years (N = 5) and 70–79 years (N = 2),
significant (positive) impact (P = 0.021) and for
these age groups were excluded from the analyses. The
Partner Relationship, living with a partner was the
age distribution and other clinical data for the remain-
only significant (positive) factor (P = 0.042). Sexual
ing 308 OSA patients are presented in Table 1. Mean
Life was significantly negatively affected by BMI
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
Table 2. Scores from Fugl-Meyer LiSat for obstructive sleep
ciated with cardiovascular medication (P = 0.008),
psychopharmaca (P = 0.010) and age (P = 0.001).
No significant associations were found for OverallSatisfaction. Discussion
The present study is, to our knowledge, the first inves-
tigation of general sexual activity and functional sexual
aspects in patients with a confirmed diagnosis of OSA
compared with age-matched controls. Most other
studies focus on (self-reported) erectile function,
whereas the present study also deals with self-reported
sexuality in a wider context. Our results show that male
patients with OSA severe enough to make them candi-
dates for CPAP treatment score worse than control
groups not only on questions regarding health in
general but also on questions regarding general and
The strength of our study is that it is based on a series
of patients with a verified diagnosis of OSA with an age
Statistical analysis performed with t-test. Scale is from 1 to 6, with
ranging from 30 to 69, a group that we consider rep-
higher scores indicating greater satisfaction.
resentative of the typical OSA patient seen in sleep
clinics. These findings are not explained by the AHI,
†Normative Swedish sample of male (8).
which is the most commonly used index of severity ofOSA.
The socio-demographic data of our patients were
(P = 0.032), and positively affected by being in a rela-
compared with the Danish Health and Morbidity
tionship (P = 0.032). No other variables showed any
Survey (SUSY2000) based on a random sample of 8188
Danish male citizens aged 16 or older (10). More of ourOSA patients (84%) lived with a partner versus SUSY2000 (68%). The percentage of patients living with a
partner (84%) may reflect a selection bias, because
The BSFI (Sexual Drive, Erection, Ejaculation, Sexual
OSA patients living alone may go undetected. Other
Problem Assessment, Total Score of the aforemen-
socio-economic aspects that might influence sexual life
(income, social status) were not covered by our ques-
showed that OSA patients generally scored worse
tionnaire. However, our results are based on a consecu-
than the control group of comparable age (age 30–69,
tive series of sleep apnoea patients from Denmark’s
n = 1185) (Fig. 1). To assess the specific impact on
largest sleep clinic. The public health care system of
OSA patients of BMI, AHI, ESS, being in a relation-
Denmark ensures that all patients are entitled to
ship, education, employment and medication, a
receive adequate investigations and treatment without
regression analysis was performed. A significant nega-
any financial restrictions. We therefore believe that the
tive relationship was found between Sexual Drive
socio-economic profile of our patients is likely to be
and cardiovascular medication (P = 0.015). Erection
representative of the Danish population as a whole. It
showed a significant negative association with
is difficult to draw any firm conclusions concerning
employment (P = 0.038) and age (P = 0.001). Ejacula-
the true prevalence of comorbidities from the data
tion showed negative association with cardiovascular
concerning cardiovascular or psychopharmacological
medication (P = 0.016), psychopharmaca (P = 0.043)
medication. However, it seems reasonable to assume
and age (P = 0.017). Sexual Problem Assessment
that OSA patients who already have regular contacts
showed negative association with cardiovascular
with the health care system also have a shorter way to
medication (P = 0.012), psychopharmaca (P = 0.010)
referral for OSA investigations, thereby creating a
and age (P = 0.001). Total Score was negatively asso-
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
Figure 1. Age-related scores from the Brief Sexual Function Inventory for OSAS male patients: n = 308 and control group n = 1185. Statistical analysis performed with t-test. OSAS, obstructive sleep apnoea syndrome. Values are expressed as mean. Scored from 0 to 4, with higher scores indicating better function. *P < 0.05, **P < 0.005, ***P < 0.0005. Fugl-Meyer LiSat
OSA patients considered their Life as a Whole
We found that age had a negative association with
(Fugl-Meyer LiSat) to be worse than the control
Sexual Drive, Erection, Ejaculation, Sexual Problem
groups. This may be a consequence of disturbed
Assessment and Total Score on the BSFI. Only Overall
sleep. It has been reported that disturbed sleep
Satisfaction (BSFI) showed no significant relationship
may have a negative effect on immune response and
with age. These findings are consistent with the results
affect mood (11). When looking at specific sexual
of O’Leary et al., who found an age-related decrease in
items, we found that sexual life was negatively asso-
erectile function and sexual functioning using BSFI
ciated with BMI. This finding corresponds with the
(5). Chung et al. conclude that obesity in itself does not
results in Kolotkin et al., who found that a higher
seem to be an underlying factor for erectile dysfunc-
BMI was associated with greater impairment in
tion, but does increase the risk of vasculogenic impo-
sexual quality of life (12). However, we found no rela-
tence through the development of chronic vascular
tionship with AHI or ESS measures that are com-
diseases of diabetes, hypertension, heart diseases and
monly used to assess the severity of sleep apnoea
hyperlipidaemia (13). Although we could not demon-
strate any association with diabetes, our results con-
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
cerning BMI and cardiovascular medication support
Maribo Medico for an unconditioned financial grant
the conclusion by Chung et al. (13). In addition, and to
our knowledge, this had not been investigated in OSA
We thank Axel Fugl-Meyer for personal communi-
patients before; psychopharmaca also has a negative
cation and giving us access to unpublished details from
association with Ejaculation, Sexual Problem Assess-
A separate analysis only for those patients not on
medication (thus eliminating a powerful confounding
References
factor) was performed. This analysis also failed toreveal any effect of AHI or ESS on any of the outcome
1. Luboshitzky R, Aviv A, Hefetz A, et al. Decreased
variables. Categorization of AHI with a cut-off of 30
pituitary-gonadal secretion in men with obstructive sleep
gave essentially similar results to treating AHI as a con-
apnea. J Clin Endocrinol Metab. 2002;87: 3394–8.
tinuous variable, i.e. no effect. Our findings are at vari-
2. Margel D, Cohen M, Livne PM, et al. Severe, but not
ance with the results of Margel et al., who found a
mild, obstructive sleep apnea syndrome is associated with
relationship between severity of OSA and the degree of
erectile dysfunction. Urology. 2004;63: 545–9.
3. Westheimer RK, Lopater S. Human Sexuality, (2nd
erectile dysfunction (2). An explanation may be that
Edition). Baltimore: Lippincott Williams & Wilkins,
our recruitment process included only those patients
who were scheduled for CPAP treatment. Some of
4. Gonςalves MA, Guilleminault C, Ramos E, et al. Erectile
these patients were, after physicians’ evaluation, pre-
dysfunction, obstructive sleep syndrome and nasal CPAP
scribed CPAP because of significant symptoms of
treatment. Sleep Med. 2005;6: 333–9.
OSA, even though they had only a moderate or even
5. O’Leary MP, Rhodes T, Girman CJ, et al. Distribution of
low AHI. These patients were therefore likely to have
the Brief Male Sexual Inventory in community men. Int J
more symptoms or comorbidities, which might affect
the outcome on sexual questionnaires.
6. Hanak V, Jacobson DJ, McGree ME, et al. Snoring as a
Nevertheless, these data point to the fact that a
risk factor for sexual dysfunction in community men. J
simple quantitative relationship between AHI and
7. Johns MW. A new method for measuring daytime
sexual dysfunction (lack of well-being, decreased
sleepiness: the Epworth Sleepiness Scale. Sleep. 1991;14:
general well-being, sexual problem) is an oversimplifi-
cation. Sexual dysfunction in OSA is a complex
8. Fugl-Meyer AR, Melin R, Fugl-Meyer KS. Life satisfaction
problem; for example, obesity and comorbidity may
in 18- to 64-year-old Swedes: in relation to gender, age,
interact through hormonal, vascular or psycho-
partner and immigrant status. J Rehabil Med. 2002;34:
9. Mykletun A, Dahl AA, O’Leary MP, et al. Assessment of
male sexual function by the Brief Sexual Function
Conclusion
Inventory. BJU Int. 2005;97: 316–23.
The important finding in this study is that although
10. Kjøller M, Rasmussen NK. Danish Health and MorbiditySurvey 2000. Copenhagen, Danish Government of Public
OSA per se seems to be associated with an impairment
in most aspects of male sexuality, not only erectile
11. Kawahara S, Akashiba T, Akahoshi T, et al. Nasal CPAP
dysfunction, the degree of sexual problems was not
improves the quality of life and lessens the depressive
quantitatively related with AHI but rather with age and
symptoms in patients with obstructive sleep apnea
comorbidity and, to some extent, with obesity and
syndrome. Intern Med. 2005;44: 422–7.
12. Kolotkin RL, Binks M, Crosby RD, et al. Obesity and
sexual quality of life. Obesity. 2006;14: 472–9.
13. Chung WS, Shon JH, Park YY. Is obesity an underlying
Acknowledgements
factor in erectile dysfunction? Eur Urol. 1999;36:
We thank Dr Jan Ovesen and the staff in ScanSleep for
their invaluable help in collecting data. We thank
The Clinical Respiratory Journal (2009) • ISSN 1752-6981
Current management of glaucoma Kenneth Schwartza and Donald Budenzb Purpose of review Introduction This study reviews current concepts in the goals of glaucomaThe management of glaucoma typically proceeds fromtherapy, interventional sequence, and options for theinterventions that are the safest and the least invasive, tomanagement of glaucoma in light of recent clinical trials. those
Departamento de Lenguaje y Comunicación Profesoras: Rebeca Muñoz y Joselinne Sepúlveda Guía de actividades: USO DE V y B NOMBRE: _______ CURSO: 1º Medio ___ FECHA: __. 0 . 11 La pronunciación “V” y “B” es idéntica en el español. Su distinción es sólo de carácter ortográfico y tiene su causa en la etimología de las palabras. Completar : Ad__erso Ad__ers
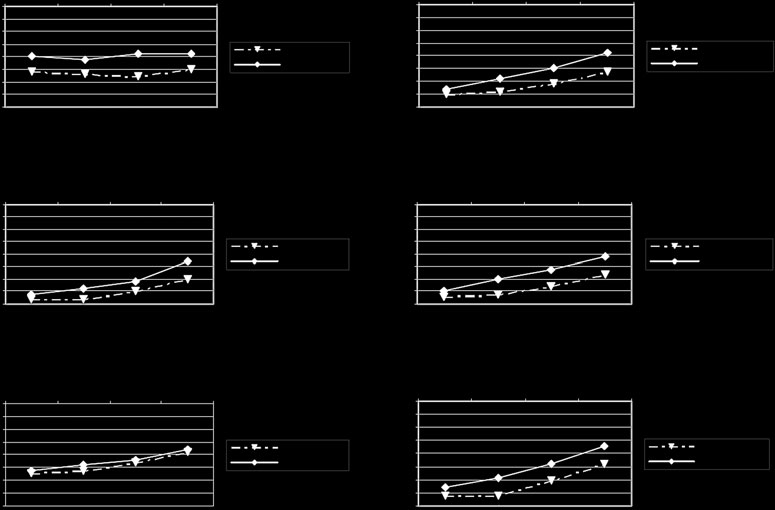 Figure 1. Age-related scores from the Brief Sexual Function Inventory for OSAS male patients: n = 308 and control group n = 1185.
Figure 1. Age-related scores from the Brief Sexual Function Inventory for OSAS male patients: n = 308 and control group n = 1185.