Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Drug dependence treatment in prison and upon release
Satellite on HIV/AIDS in Prison Settings 18th International Conference to Reduce Drug Related Harm Warsaw, Poland May 13, 2007
3-6 weeks inpatient hospital followed by extended
out-patient talk therapy and/or 12 step programs
Pts. withdrawn from drugs under physician’s care,
in-patient or out-patient (precursor to treatment)
Drug education/admonition/group & individual
Drug Substitution Treatment (opioid agonist
MethadoneBuprenorphineCodeineSlow-release morphineOpiumHeroinNaltrexone*
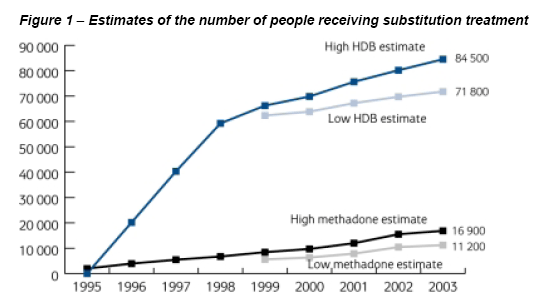
Opioid substitution therapy for illicit
Can be used as a detox. tool in tapering
Long-acting (typically 24 hours) Blocks effects of other opioids like heroin Stops cravings: biggest factor in relapse
Methadone Maintenance treatment is the most
effective treatment available for heroin dependent
injecting drug users (IDUs) for reducing
Mortality (Capelhorn, et al., 1994)
Heroin consumption (Gottheil, et al, 1993)
Criminality (Newman, et al., 1973) and
HIV infection (Blix and Gronbladh, 1981; Reducing the spread of HIV and other infections. Injecting drug users are over- represented in prisons and they are at higher risk for contracting and spreading infections. Continuity of medical care. The increasing number of IDUs in community-based methadone programs means more prisoners in opioid withdrawal.
Pregnant IDUs at high risk. Overdose Prevention. Highest risk of overdose is after periods of abstinence or reduced use, incarceration.
The introduction or expansion of methadone in prisons has
been recommended by a number of prominent medical &
UK’s Advisory Council on the Misuse of Drugs, 1993
NIH Consensus Development Panel on Effective
Treatment of Heroin Addiction, 1997 (U.S.A.)
World Health Organization/United Nations Office of
Drugs and Crime, Joint United Nations Programme on
National Institute on Drug Abuse, 2006 (U.S.A.)
Preventing HIV Infection Among Injecting Drug Users in High Risk Countries: An Assessment of the Evidence Commission by Global Fund and Gates Foundation Released on: September 15, 2006
reduce the risk of transmission of HIV”
“We do not end [the Report] with ‘More
research is needed.’ … We say instead
Prisoners should have access to the same
medical care and health care services as
External professional standards of care
Additional Sources: Dolan 2001, EMCDDA 2002
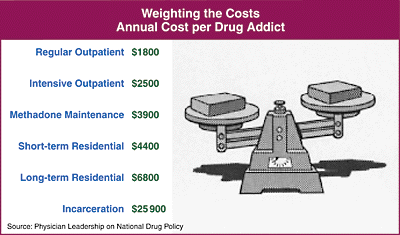
MMT costs approx. $4000 per patient per
and improves social productivity, all of
which serve to reduce the societal costs
of drug addiction, i.e. re-incarceration,
Cost benefit analyses indicate savings of
1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 19951997 1999
Patients often stop using opioids, but if
Caplehorn 1996, Sporer 1999, 2003, Auriacombe 2004,Stancliff 2007
About 2% of heroin users die each year -
1999: most common cause of death men age
25-54 in Portland OR and several other cities
Incarceration Hospitalization Drug treatment/detox
Primarily other CNS depressantsCocaine is involved in nearly 40% of NYC
Overdose is more likely in the presence of
significant illness: cirrhosis, AIDS, coronary
Major changes in opioid supply: >1000 deaths
http://www.whitehousedrugpolicy.gov/news/fentnyl%5Fheroin%5Fforum
Most often it’s dependent long term users
with 5- 10 years of experience rather than
hours- the stereotype “needle in the arm”
Overall mortality: 2.5 times than expectedFirst 2 weeks: 12.7 times than expected
Opioids: 60% Cocaine and other stimulants: 74%
Opioid antagonist which reverses opioid related
sedation and respiratory depression and may cause
Displaces opioids from the receptors, then occupies
http://www.ofdt.fr/BDD/publications/docs/eftaack6.pdf
e.g., long-term Rx in New York City 1970-72
GRAND TOTAL 12,450 52,782
Newman J. Pub. Health Policy 6(4):526-538 (1985)
End 1974: one “pilot” program, 500 patients
End 1975: approximately 2,000 enrolled
End 1976: approximately 10,000 enrolled
(Admissions to voluntary in-patient drug-free programmes stable
Newman J. Pub. Health Policy 6(4):526-538 (1985)
* Gölz, J.: Stellungnahme der DGS - Deutsche Gesellschaft für Suchtmedizin zur
"Berliner Erklärung". In: Suchtmedizin in Forschung und Praxis 2006;8(3):156
Ralf Jurgens, WHO, UNODC, UNAIDSRobert Newman, MD International Center
Formulary Drug List - MINNESOTA 6/9/2011 If you have any questions regarding pharmaceutical pricing, please contact PharmaCorr for clarification. 6705 Camille St; Oklahoma City , OK 73149 Toll Free: 888-321-7774 Local: 405-670-1400 Fax: 888-200-77746002 Corporate Way, Corporate Cntr North II; B; Indianapolis, IN 46278 Toll Free: 800-259-3067 Local: 317-299-3426 Fax: 800-259-3066 Fo
t. nr 755429 januari 2007, Rehn & Co: 040 - 611 90 11Riksförbundet för Mag- och Tarmsjuka (RMT), telefon 08-642 42 00 eller www.magotarm.seEuropeiska föreningen för patienter med IBD: www.efcca.org Denna folder har tagits fram som en service till sjukvården i samråd med Rikard Svernlöv, Specialistläkare, Universitetssjukhuset i Linköping. • Hur stor del av min tarm är in�
 MMT costs approx. $4000 per patient per
and improves social productivity, all of
which serve to reduce the societal costs
of drug addiction, i.e. re-incarceration,
Cost benefit analyses indicate savings of
MMT costs approx. $4000 per patient per
and improves social productivity, all of
which serve to reduce the societal costs
of drug addiction, i.e. re-incarceration,
Cost benefit analyses indicate savings of
 1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 19951997 1999
Patients often stop using opioids, but if
Caplehorn 1996, Sporer 1999, 2003, Auriacombe 2004,Stancliff 2007
About 2% of heroin users die each year -
1999: most common cause of death men age
25-54 in Portland OR and several other cities
Incarceration Hospitalization Drug treatment/detox
Primarily other CNS depressantsCocaine is involved in nearly 40% of NYC
Overdose is more likely in the presence of
significant illness: cirrhosis, AIDS, coronary
Major changes in opioid supply: >1000 deaths
http://www.whitehousedrugpolicy.gov/news/fentnyl%5Fheroin%5Fforum
Most often it’s dependent long term users
with 5- 10 years of experience rather than
hours- the stereotype “needle in the arm”
Overall mortality: 2.5 times than expectedFirst 2 weeks: 12.7 times than expected
Opioids: 60% Cocaine and other stimulants: 74%
1969 1971 1973 1975 1977 1979 1981 1983 1985 1987 1989 1991 1993 19951997 1999
Patients often stop using opioids, but if
Caplehorn 1996, Sporer 1999, 2003, Auriacombe 2004,Stancliff 2007
About 2% of heroin users die each year -
1999: most common cause of death men age
25-54 in Portland OR and several other cities
Incarceration Hospitalization Drug treatment/detox
Primarily other CNS depressantsCocaine is involved in nearly 40% of NYC
Overdose is more likely in the presence of
significant illness: cirrhosis, AIDS, coronary
Major changes in opioid supply: >1000 deaths
http://www.whitehousedrugpolicy.gov/news/fentnyl%5Fheroin%5Fforum
Most often it’s dependent long term users
with 5- 10 years of experience rather than
hours- the stereotype “needle in the arm”
Overall mortality: 2.5 times than expectedFirst 2 weeks: 12.7 times than expected
Opioids: 60% Cocaine and other stimulants: 74%
 Opioid antagonist which reverses opioid related
sedation and respiratory depression and may cause
Displaces opioids from the receptors, then occupies
Opioid antagonist which reverses opioid related
sedation and respiratory depression and may cause
Displaces opioids from the receptors, then occupies
 http://www.ofdt.fr/BDD/publications/docs/eftaack6.pdf
e.g., long-term Rx in New York City 1970-72
GRAND TOTAL
http://www.ofdt.fr/BDD/publications/docs/eftaack6.pdf
e.g., long-term Rx in New York City 1970-72
GRAND TOTAL