Kamagra repose sur le sildénafil comme principe actif, avec un mode d’action identique à celui du Viagra. La forme galénique en gel oral permet une absorption plus rapide et une concentration plasmatique maximale plus précoce que les comprimés. Le mécanisme implique l’inhibition compétitive de la PDE5, entraînant une relaxation musculaire lisse locale et une vasodilatation ciblée. La demi-vie courte, environ 4 heures, limite la durée d’action. L’élimination se fait après métabolisme hépatique, impliquant majoritairement le CYP3A4. L’incidence d’effets indésirables comprend céphalées, rougeurs et congestion nasale, de façon transitoire. Dans les comparatifs pharmacologiques, acheter kamagra sans ordonnance est associé aux présentations galéniques alternatives disponibles.
Decoupling of autonomic and cognitive emotional reactions after cerebellar stroke
BRIEF COMMUNICATIONS
changes in response to pertinent stimuli.6 It is not yetclear if the autonomic response occurs alone6 pre-
cedes,7 accompanies,8 or follows a cognitive appraisal.9Importantly, all theories posit a modulation of the au-
tonomic system during an emotional experience,
whether the change is primary or secondary. The abil-ity of the cerebellum to modulate autonomic reac-
Jean-Marie Annoni, MD,1 Radek Ptak, PhD,2
tions10 could partly explain its importance for emo-
Anne-Sarah Caldara-Schnetzer, MA,1 Asaid Khateb, PhD,1
responses (SCRs) to emotionally pertinent stimuli, asan index of autonomic arousal, are decreased in frontalpatients with emotional loss11 and therefore are well
Emotional blunting can be found after cerebellar lesions.
suited for the study of cerebellar patients with emo-
However, the mechanism of such a modification is not clear. We present a patient with emotional flattening and
Here, we present a patient who, after an extensive
increased risk taking after left cerebellar infarct who had
left cerebellar stroke, showed a severe emotional flat-
an impaired autonomic reactivity to negative as com- pared with positive reinforcement. This impairment was
tening. This impairment is hypothesized to result from
demonstrated by the patient’s undifferentiated skin con-
an undifferentiated sympathetic response to the valence
ductance responses to negative and positive reinforce- ment, whereas controls produced larger skin conductance responses after negative feedback. The cooccurrence of Case Report emotional flattening and undifferentiated autonomic re-
M.F., an overweight and hypertensive 53-year-old right-
actions to positively and negatively valenced stimuli
handed patient was admitted because of unusual headaches,
strengthens the role of the cerebellum in the modulation
vomiting, instability, and progressive stupor (for approxi-
of the autonomic responses.
mately 48 hours). On admission, he was bradycardiac, scored14 at the Glasgow coma scale, and showed Parinaud’s syn-
drome and left hemiataxia at the finger-to-nose and heel-to-shin tests. Pupillary, corneal, and oculomotor reflexes werenormal. Computed tomography scan showed a large left cer-
Although emotional disturbances are typically found
ebellar stroke including the left fastigial nucleus, with mass
after limbic, particularly amygdalar or ventral frontal,
effect on the fourth ventricle and obstructive supratentorial
damage,1 there is growing evidence for a cerebellar
hydrocephalus. After lateral cerebellar aspiration (at 24
contribution to affective reactions.2 Emotional flatten-
hours), Parinaud’s syndrome and hemiataxia disappeared af-
ing seems to correlate with the extent of cerebellar de-
ter 2 days. After a subsequent reintervention (10 days later)
generation.3 Blunting of affect and inappropriate be-
for an abscess in the epidural layer under the craniotomy
havior have been observed, together with executive,
scar, neurological recovery was flawless. It was then that
visuospatial, and memory dysfunction, after posterior
M.F.’s wife noticed that her husband appeared more apa-
and vermian cerebellar lesions.4 However, the neural
thetic and “detached from life” than before the stroke. Post-
mechanisms underlying cerebellar modulation of emo-
operative magnetic resonance imaging (Fig 1) indicated leftposterior inferior and anterior inferior cerebellar infarcts.
tional experience remain poorly understood.
Three months after surgery, the patient reported lack of
Theories of emotional experience have distinguished
recent memory, difficulties following complex conversations,
different possible mechanisms.5 Referring to James’
and difficulties making decisions in daily life. However, his
classic example (seeing the bear, running, experiencing
most persistent complaint concerned the loss of emotions.
fear), visceral feedback hypothesis postulates that emo-
He could neither feel sadness, nor anger or joy. The sensa-
tional experience results from the perception of visceral
tion of pain and hunger was diminished. He also declaredthat other persons’ emotional states had lost importance forhim (“Before my stroke, when a person of the family wassuffering, it was as if a part of myself was ill. Now, it is asimple fact, like something written in a newspaper.”) Self-
From the Departments of 1Neurology, 2Neurorehabilitation, and
3Liaison Psychiatry, Geneva University Hospital, Geneva, Switzer-
evaluation of his life situation was marked by affective indif-
ference. At 10 months, reports remained unchanged, partic-ularly concerning loss of emotions and decreased decision-
Received Aug 29, 2002, and in revised form Jan 21, 2003. Acceptedfor publication Jan 27, 2003;
evaluations (Table 1) were normal. Neuropsychological eval-uation showed slowed reaction times and a relatively lowperformance in tests of cognitive flexibility and interference
Address correspondence to Dr Annoni, Department of Neurology,
control (Table 2). M.F.’s facial expressions (recorded during
Geneva University Hospital, 24 Rue Micheli-du-Crest, CH-1211Geneva 14, Switzerland. E-mail: [email protected]
verbal recall of his own previously experienced emotional re-
actions of joy, anger, and sadness) were analyzed using theFacial Action Coding System.12 They were undifferentiated,joyful most of the time, and unaffected by the emotionalcontent of the discourse. To assess M.F.’s vocal expression ofemotions, his voice was acoustically analyzed.13 Althoughtalking about joyful experiences produced a higher level ofvocal arousal, sad and angry experiences produced undiffer-entiated responses. M.F. scored 13 of 21 at the HospitalAnxiety and Depression scale,14 suggestive of moderate de-pression. Blood tests, including measures of ACTH andTSH levels, were normal, suggesting normal hypothalamicfunction. Antidepressive medication (citalopram 20mg) wasstopped after 6 months, because it changed neither apathynor depression. A subsequent cognitive therapy focusing onemotional reactions and prosody improved his affective pros-ody and social integration, but not depression (11/21) norperception of emotional experiences. Results M.F. consented to participate to this investigation ad- dressing the following questions: (1) Does he have an intact semantic knowledge of emotional stimuli? (2) Does he have normal autonomic reactions to emotion- ally pertinent stimuli?
M.F.’s semantic knowledge was first assessed using a
picture categorization task (240 pictures selected fromthe International Affective Picture System, rated forarousal and affective valence15). Pictures, depictingemotionally positive and negative situations (eg, beau-tiful scenes, disaster, death) were either low arousal(mean, 4.3 Ϯ 0.8; n ϭ 120) or high arousal (mean,6.3 Ϯ 0.6; n ϭ 120). Images were pseudorandomlypresented on the computer screen, and M.F. decidedwhether they represented positive or negative situa-tions. His performance (19/240 errors) was comparableto that of a control group (mean, 32 Ϯ 11.5 errors;n ϭ 11, 7 women, age, 29 Ϯ 6). Categorization offacial expressions into happy, sad, or neutral16 was per-fect. Auditory categorization of recorded voices express-ing sadness, joy, or anger was also correct,17 indicatingthat M.F.’s semantic knowledge of emotional stimuliwas intact.
To evaluate M.F.’s autonomic responses, SCRs were
measured in response to an orientation stimulus (a sud-den noise) and to his first name appearing unexpect-edly among neutral words (Fig 2A). In both tasks, hisSCRs were within the range of control subjects (n ϭ10; 5 women; age, 45 Ϯ 9 years), suggesting that hisautonomic system responded normally to stimuli with
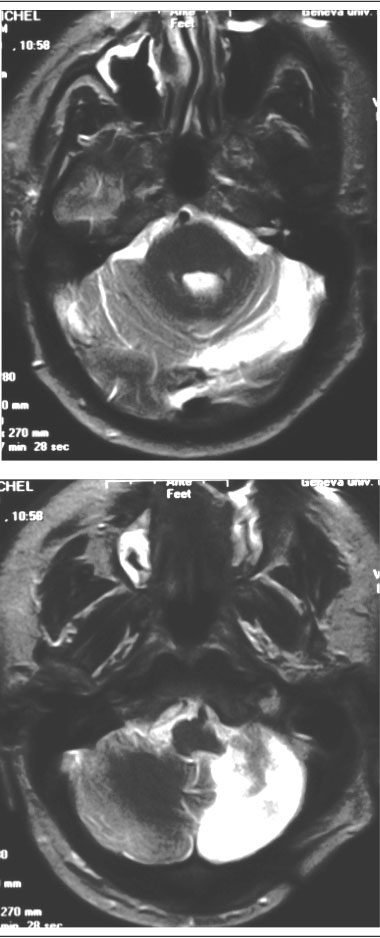
Fig 1. Transverse magnetic resonance imaging (MRI) sections
high salience (Z-score ϭ Ϫ0.51 for sudden noise and
(at 21mm interval) of the cerebellar lesion 3 months after thestroke (Transverse 7mm thick fast spin echo T2). MRI images
SCRs also were collected during two other experi-
demonstrate that M.F.’s stroke included the territories of bothanterior inferior and posterior inferior left cerebellar arteries.
ments. The first was a conditional learning task requir-
The dentate nucleus seems partly preserved. No other lesion
ing M.F. to learn four form-figure pairs across 32 tri-
als; feedback was given after each correct and wrongchoice. M.F. showed normal learning (Z-score ϭ0.59), and SCRs were comparable to those of controls
Annoni et al: Emotional Changes after Cerebellar Stroke
Table 1. Bedside Testing of M.F.’s Autonomic Functions
BP response to standing up (from supine)c
aDiameter of each pupil in shadow/diameter after exposure to the light of a pocket electric torch.
bBlood pressure after 10 minutes of lying down; BP ϭ blood pressure.
cMeasured after 1 minute of standing upright (patient moves from supine to standing in about 3 seconds).
dConcerning the pulse rate, the low cardiac frequency is probably related to propanolol intake for blood pressure control.
eAverage difference between maximal and minimal heart during a forced breathing with a frequency of 6 breath/min) is moderately low. However the Valsalva index (defined by Wieling24 as the longest R-R interval in phase 4 reflex bradycardia/shortest R-R interval in phase 2compensatory increase in heart rate, when the patient exhales against a resistance of 40 mm Hg for 20 seconds) was normal, suggestive of intactcardiovascular parasympathetic reactive ability (for age-matched controls, see Wieling24). Table 2. Neuropsychological Profile of Patient M.F. 10
The second assessment involved the “gambling”
task,11 which requires subjects to select a card fromone of four stacks representing advantageous (ie, asso-
ciated with small money gain but an even smaller loss)or disadvantageous (associated with a large gain but an
even larger loss). Patients with ventromedial damage
consistently preferred the disadvantageous cards and
showed diminished SCRs preceding their choice.11
Like these patients, M.F. chose more frequently disad-
vantageous (62/100) than advantageous decks (38/100)
and thus gradually lost his money. Afterward, he re-
ported that some decks seemed worse than others,
without being able to specify why. His disadvantageous
choices did not appear to be caused by a lack of antic-
ipation, since, as previously reported in controls,11 his
SCRs preceding disadvantageous choices were signifi-
cantly higher (0.24S) than SCRs preceding advanta-
geous choices (0.17S; p Ͻ 0.05). In contrast, M.F.
did not show differential responses to low (0.42S)
found in the conditional learning task. Discussion
The cerebellar cognitive-affective syndrome4 presented
by this patient appears particularly interesting in view
The Boston Naming 34 items is a shortened French version of orig-
of his self-reported inability to experience emotion and
of his moderate depression. Our investigation indicates
RAVLT ϭ Rey Auditory Verbal Learning Test; RVDLT ϭ Rey
that M.F.’s emotional flattening was caused neither by
Visual Design Learning Test; d2 ϭ d2 attention test (1982 Ver-
an inability to cognitively evaluate emotional situations
ϭ Trail Making Test; WCST ϭ Wisconsin Card Sort-
ing Test (Nelson’s short version).
nor by a general autonomic dysfunction. Actually, bothhis Valsalva index and his SCRs to sudden noise, to hisname, and before disadvantageous choices (gambling
(n ϭ 10; 5 women; age, 45 Ϯ 9 years), indicating a
task) were normal. These findings indicate that arousal
preserved overall reactivity. However, whereas healthy
responses to salient stimuli were unaffected. The major
participants showed higher SCRs to feedback for
difference between M.F. and healthy subjects con-
wrong (0.94S) than for correct (0.29S) choices
cerned the failure of his autonomic system to generate
(Wilcoxon Z ϭ 2.4; p Ͻ 0.05), M.F. did not respond
different arousal responses to positive and negative sit-
differently to these two conditions (0.42 and 0.39S,
uations. In the conditional learning task, based on cog-
nitive deduction, absence of differential autonomic re-
Fig 2. Mean (Ϯ SEM) skin conductance responses (SCRs) of control subjects and patient M.F. in two tasks. (A) The pattern ofM.F.’s SCR to the critical (first name, white histograms) and uncritical stimuli (neutral words, dark histograms) is comparable tothat of control subjects. (B) SCRs in the conditional learning task after positive feedback for correct responses (unshaded bars) ornegative feedback for wrong responses (shaded bars). Unlike control subjects, M.F. did not show differential responses in these twoconditions. uS ϭ microsiemens.
actions to positive and negative outcomes did not
tional imaging studies proposed the involvement of the
interfere with M.F.’s performance. In contrast, in the
left cerebellum in autonomic arousal and in SCR gen-
gambling task, where decisions are hypothesized to rely
eration.22 In line with the above evidence, but also
on experienced somatic arousal,11 SCR undifferenti-
with works suggesting a role for the cerebellum in de-
ated responses to positive and negative outcomes were
pression,23 this single case investigation points to a role
associated with behavioral failure. Interestingly, despite
for the cerebellum in the generation of emotionally
his failure in the gambling task, M.F. generated normal
congruent autonomic reactions. Additional group stud-
anticipatory SCRs. This pattern, being the inverse of
ies are needed to confirm this interpretation.
that observed after ventromedial damage,11 suggests apossible independence between self-generated anticipa-tory autonomic activity and reactions to external stim-
This work was supported by the Swiss National Science Foundation
uli (externally provided feedback). We hypothesize that
(31-61680-00, J.-M.A., and 3100-100156, R.P.).
M.F.’s autonomic inability to react differentially to
We thank A. Schider for providing the electrodermal setting.
positively and negatively valenced external stimuli con-stitutes a possible explanation for his reported loss of toexperience emotions. References
Although alterations of SCRs in cerebellar patients
1. Eslinger P, Damasio A. Severe disturbance of higher cognition
are not well documented, several studies suggested the
after bilateral frontal lobe ablation: patient EVR. Neurology
involvement of the cerebellum in autonomic function.
Autonomic dysfunction was shown to increase in cer-
2. Reiman E, Lane R, Ahern G, et al. Neuroanatomical correlates
ebellar atrophy.18 Electrical cerebellar stimulation was
of externally and internally generated human emotion. Am JPsychiatr 1997;154:918 –925.
shown to induce autonomic arousal and predatory be-
3. Gutzmann H, Kuhl K. Emotion control and cerebellar atrophy
havior19 and to modulate ventrolateral medullary ad-
in senile dementia. Arch Gerontol Geriatr 1987;6:61–71.
renergic vasomotor neurons.20 Cerebellar damage was
4. Schmahmann J, Sherman J. The cerebellar cognitive affective
shown to alter autonomic cardiovascular responses.10
Finally, in accordance with anatomical findings dem-
5. Heilman K. Emotion and the brain: a distributed modular net-
work mediating emotional experience. In: Zeidel D, ed. Neu-
onstrating dense connections between the fastigial nu-
ropsychology. San Diego: Academic Press, 1994.
cleus and the hypothalamus (strongly implicated in
6. James W. Principles of psychology. New York: Dover, 1890/
sympathetic and parasympathetic modulation,)21 func-
Annoni et al: Emotional Changes after Cerebellar Stroke
7. Schacter E, Singer J. Cognitive, social and physiological deter-
minants of emotional state. Psychol Rev 1962;69:379 –399.
8. Cannon W. The James-Lange theory of emotions. Am J Psy-
9. Scherer K. On the nature and function of emotion: a compo-
nent process approach. In: Scherer K, Ekman P, eds. Ap-proaches to emotion. Hillsdale, NJ: Lawrence Erlbaum Associ-
Tejal N. Mitchell, MRCP,1,2 Samantha L. Free, PhD,1,2
10. Chen C, Williams J, Lutherer L. Cerebellar lesions alter
autonomic responses to transient isovolaemic changes in arte-
rial pressure in anaesthetized cats. Clin Auton Res 1994;4:
11. Bechara A, Damasio H, Damasio A. Different contributions of
the human amygdala and ventromedial prefrontal cortex to
Veronica van Heyningen, PhD,3and Sanjay M. Sisodiya, MRCP, PhD1,2
decision-making. J Neurosci 1999;19:5473–5481.
12. Ekman P, Friesen W. Facial Action Coding System. Consulting
13. Scherer K, Zei B. Vocal indicators of affective disorders. Psy-
Identification of genes involved in human cerebral devel-
chother Psychosom 1988;49:179 –186. opment is important for our understanding of disorders
14. Zigmond A, Snaith R. The Hospital Anxiety and Depression
with potential neurodevelopmental causes such as epi-
Scale. Acta Psychiatr Scand 1983;67:361–370. lepsy and learning disability. Murine models suggest that
15. Lang P, Bradley M, Cuthbert B. International Affective Picture
PAX6 plays a key role in human brain development.
System (IAPS): instruction manual and affective ratings. Techni-
With magnetic resonance imaging in 24 humans het-
cal Report A-4. The Center for Research in Psychophysiology:
erozygous for defined PAX6 mutations, we demonstrated widespread structural abnormalities including absence of
16. Bruyer R, Schweich M. A clinical test battery of face processing. the pineal gland and unilateral polymicrogyria.
17. Zei B, Archinard M. The role of autonomic balance in experi-
encing emotions. In: Kaszniak A, ed. Emotions, qualia, andconsciousness. Singapore, New Jersey, London, Hong Kong:World Scientific Publishing, 2001:278 –284. PAX6 is a highly conserved developmentally regulated
18. Smith GD, Mathias CJ. Differences in cardiovascular responses
gene, encoding a transcription factor containing two
to supine exercise and to standing after exercise in two clinical
DNA-binding domains, a paired domain, and a home-
subgroups of Shy-Drager syndrome (multiple system atrophy).
odomain. PAX6 is known to influence cellular prolif-
J Neurol Neurosurg Psychiatr 1996;61:297–303.
eration, neuronal migration, and axonal guidance in
19. Snider R, Maiti A. Cerebellar contributions to the Papez cir-
the brain.1–5 Mice homozygous for mutations in the
cuit. J Neurosci Res 1976;2:133–146.
perfectly conserved Pax6 gene die neonatally, with a
20. Spyer KM. Central nervous control of the of the cardiovascular
system. In: R. B, J. MC, eds. Autonomic failure. 3rd ed. Ox-
wide variety of neurodevelopmental abnormalities, in-
ford, UK: Oxford University Press, 1992:61.
cluding polymicrogyria, subcortical heterotopia, and
21. Haines D, Dietrichs E, Mihailoff G, McDonald E. The
absence of the corpus callosum, olfactory bulb, cerebel-
cerebellar-hypothalamic axis: basic circuits and clinical observa-
lar vermis and pineal gland,6,7 and anophthalmia and
tions. Int Rev Neurobiol 1997;41:83–107.
absence of nasal structures and the pancreas. Murine
22. Critchley H, Elliott R, Mathias C, Dolan R. Neural activity
heterozygotes have microphthalmia, iris hypoplasia,
relating to generation and representation of galvanic skin con-
cataracts and corneal anomalies, and olfactory bulb and
ductance responses: a functional magnetic resonance imaging
cerebral abnormalities, which are much less severe than
study. J Neurosci 2000;20:3033–3040.
23. Schmahmann JD. The role of the cerebellum in affect and psy-
chosis. J Neurolinguistics 2000;13:189 –214.
24. Wieling W. Noninvasive continuous recording of heat rate and
From the 1Department of Clinical and Experimental Epilepsy, In-
blood pressure in the evaluation of the neurocardiovascular con-
stitute of Neurology, University College London, London; 2Nation-
trol. In: Bannister R, Mathias ChJ, MC, eds. Autonomic fail-
al Society for Epilepsy, Buckinghamshire; 3MRC Human Genetics
ure. 3rd ed. Oxford: Oxford University Press, 1992:298.
Unit, Western General Hospital, Edinburgh; 4Bristol Eye Hospital,Bristol; and 5Division of Inherited Eye Disease, Institute of Oph-thalmology, London, United Kingdom.
Received Oct 7, 2002, and in revised form Jan 28, 2003. Acceptedfor publication Jan 30, 2003.
(www.interscience.wiley.com). DOI: 10.1002/ana.10576
Address correspondence to Dr Sisodiya, Department of Clinical andExperimental Epilepsy, Institute of Neurology, University CollegeLondon, Queen Square, London WC1N 3BG, United Kingdom. E-mail: [email protected]
"Abstracts der Vorträge und Seminare geordnet nach ErstreferentInnen in alphabetischer Reihenfolge" Einreichung als: Vortrag Topic: C - Orale Chirurgie 10/1/2009 OCMR Session 06 von 15:15 bis 16:00 Konzept einer eingriffsadäquaten, standardisierten Schmerztherapie für die Praxis Dr. Stephan Acham Universitätsklinik für Zahn-, Mund- und Kieferheilkunde Graz Au
POLICY FOR WORKING ALONE This document provides advice for all teaching and support staff in mainstream, special and voluntary aided schools (as adopted) who regularly, or on an occasional basis, work alone with children, young people or adults. Working alone occurs in a wide range of different circumstances and it is recognised that it can present particular difficulties and concerns. The pu
 actions of joy, anger, and sadness) were analyzed using theFacial Action Coding System.12 They were undifferentiated,joyful most of the time, and unaffected by the emotionalcontent of the discourse. To assess M.F.’s vocal expression ofemotions, his voice was acoustically analyzed.13 Althoughtalking about joyful experiences produced a higher level ofvocal arousal, sad and angry experiences produced undiffer-entiated responses. M.F. scored 13 of 21 at the HospitalAnxiety and Depression scale,14 suggestive of moderate de-pression. Blood tests, including measures of ACTH andTSH levels, were normal, suggesting normal hypothalamicfunction. Antidepressive medication (citalopram 20mg) wasstopped after 6 months, because it changed neither apathynor depression. A subsequent cognitive therapy focusing onemotional reactions and prosody improved his affective pros-ody and social integration, but not depression (11/21) norperception of emotional experiences.
actions of joy, anger, and sadness) were analyzed using theFacial Action Coding System.12 They were undifferentiated,joyful most of the time, and unaffected by the emotionalcontent of the discourse. To assess M.F.’s vocal expression ofemotions, his voice was acoustically analyzed.13 Althoughtalking about joyful experiences produced a higher level ofvocal arousal, sad and angry experiences produced undiffer-entiated responses. M.F. scored 13 of 21 at the HospitalAnxiety and Depression scale,14 suggestive of moderate de-pression. Blood tests, including measures of ACTH andTSH levels, were normal, suggesting normal hypothalamicfunction. Antidepressive medication (citalopram 20mg) wasstopped after 6 months, because it changed neither apathynor depression. A subsequent cognitive therapy focusing onemotional reactions and prosody improved his affective pros-ody and social integration, but not depression (11/21) norperception of emotional experiences. Fig 2. Mean (Ϯ SEM) skin conductance responses (SCRs) of control subjects and patient M.F. in two tasks. (A) The pattern ofM.F.’s SCR to the critical (first name, white histograms) and uncritical stimuli (neutral words, dark histograms) is comparable tothat of control subjects. (B) SCRs in the conditional learning task after positive feedback for correct responses (unshaded bars) ornegative feedback for wrong responses (shaded bars). Unlike control subjects, M.F. did not show differential responses in these twoconditions. uS ϭ microsiemens.
actions to positive and negative outcomes did not
tional imaging studies proposed the involvement of the
interfere with M.F.’s performance. In contrast, in the
left cerebellum in autonomic arousal and in SCR gen-
gambling task, where decisions are hypothesized to rely
eration.22 In line with the above evidence, but also
on experienced somatic arousal,11 SCR undifferenti-
with works suggesting a role for the cerebellum in de-
ated responses to positive and negative outcomes were
pression,23 this single case investigation points to a role
associated with behavioral failure. Interestingly, despite
for the cerebellum in the generation of emotionally
his failure in the gambling task, M.F. generated normal
congruent autonomic reactions. Additional group stud-
anticipatory SCRs. This pattern, being the inverse of
ies are needed to confirm this interpretation.
Fig 2. Mean (Ϯ SEM) skin conductance responses (SCRs) of control subjects and patient M.F. in two tasks. (A) The pattern ofM.F.’s SCR to the critical (first name, white histograms) and uncritical stimuli (neutral words, dark histograms) is comparable tothat of control subjects. (B) SCRs in the conditional learning task after positive feedback for correct responses (unshaded bars) ornegative feedback for wrong responses (shaded bars). Unlike control subjects, M.F. did not show differential responses in these twoconditions. uS ϭ microsiemens.
actions to positive and negative outcomes did not
tional imaging studies proposed the involvement of the
interfere with M.F.’s performance. In contrast, in the
left cerebellum in autonomic arousal and in SCR gen-
gambling task, where decisions are hypothesized to rely
eration.22 In line with the above evidence, but also
on experienced somatic arousal,11 SCR undifferenti-
with works suggesting a role for the cerebellum in de-
ated responses to positive and negative outcomes were
pression,23 this single case investigation points to a role
associated with behavioral failure. Interestingly, despite
for the cerebellum in the generation of emotionally
his failure in the gambling task, M.F. generated normal
congruent autonomic reactions. Additional group stud-
anticipatory SCRs. This pattern, being the inverse of
ies are needed to confirm this interpretation.